 Supraspinatus moving under the bony arch of the scapula Common Shoulder Pains/ Injuries: Because of the tremendous range of motion required by the shoulder to preform functional everyday tasks or recreational activities, the shoulder is highly susceptible to injury. The shoulder becomes most susceptible to repetitive injury when lifting items or when the arm is placed in an overhead position. To perform these motions without injury requires unabated shoulder range of motion and optimum shoulder stability. It does not matter how “strong” your shoulder is when posture and scapular range of motion are limited, there will be a stronger potential for shoulder injuries. Below is a list of many common injuries to the shoulder. (Note- laxity and dislocations will not be addressed in this blog post) All of these injuries occur with a similar mechanical injury mechanisms and underlying causes: Impingement: A very common injury of the shoulder is what is termed as impingement. Just like the name implies, impingement of the rotator cuff muscle (supraspinatus specifically) develops when the space between the rigid coracoacromial arch (top of the shoulder blade) and the head of the humerus (arm bone) narrows. The muscles and tendons of the rotor cuff that pass through this space begin to fray and eventually may tear because they are pinched between these hard surfaces. Why does this space narrow? Anatomically, it narrows due to bony spurs, degenerative changes, or soft-tissue thickening. Functionally, the space narrows due to dysfunctional synchronicity of the rotator cuff muscles, aberrant scapular-humeral rhythm, or faulty scapular positioning during overhead arm movements. Individuals who are predisposed to impingement have several traits that can be distinguishable by even the untrained eye. First and foremost, a susceptible person’s shoulders commonly have the appearance of being rolled forward. Everyone has seen this person before in the local gym, their workouts consists of bench pressing and more bench pressing. They look great from the front, but when you look from the side, their shoulders sickout in front of their body. Anatomically, the scapula has tipped forward and the humerus no longer sits centered in the socket of the shoulder joint. Because the head of the humerus is positioned more forward and superior in position, the individual becomes more susceptible to impingement. These postural changes lead to the described narrowing of the space for the tendons of the rotator cuff, and start the impingement process. Typically, this postural fault of the shoulder stems from tightness and shorting of the chest muscles(Pec Minor) and reciprocated weakness and lengthening of the scapular muscles that normally stabilize the scapula to the ribcage. Interestingly, almost all cadaver studies show at least some type of fraying of tendons due to impingement. Some fraying is normal over a lifetime, but many people speed this process due to poor shoulder function, leading to actual tears in the rotator cuff muscles. A full tear of a rotator cuff muscle or tendon can cause full loss of strength in specific movements and may need to be surgically fixed. 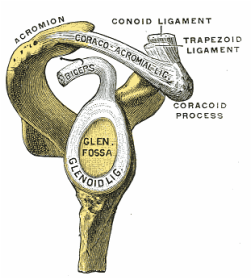 The Labrum= Glenoid Lig Bursitis In a majority of shoulder impingement cases, there is some form of bursitis involvement. Bursas are fluid filled sacs that are located throughout the body in areas of stress. They act like little pillows or shock absorbers. Most commonly they are located where a tendon travels near a bone. For example there is a bursa that is under the patellar tendon of the knee and it protects the tendon from friction with the tibia (leg bone) as it moves. There is a bursa positioned directly above the tendons of the rotator cuff in the shoulder, the “sub-acromia bursa”. When the mechanisms of impingement occur and the anatomical space narrows between the head of the humerus and scapula, not only does the tendon start to fray, but the bursa in this space is irritated. An irritated bursa will lead to an inflamed and painful bursa. When the shoulder bursa becomes inflamed, it will swell up causing even more compromise to the canal space. Many times medical doctors will inject this bursa with an anti-inflammatory to reduce the pain and swelling. But, until the mechanical stress is removed from the bursa, it will continue to become more inflamed in the future. Labral Tear - SLAP Tear The labrum gets its name from the world of architecture. In Roman architecture, a labrum was a large water-filled vessel or basin with an overhanging lip. This is actually an accurate definition of the labrum in the human shoulder. The human labrum is a layer of fibrous cartilage that surrounds the socket of bone on the scapula where the arm meets to form that shoulder joint. Because the bony socket is very shallow, the labrum adds extra depth to the socket, keeping the shoulder joint more centrated. Just like in Roman architecture, the labrum has an overhanging lip that extends around the ball head of the shoulder. The labrum in the shoulder is what we refer to as a “passive stabilizer”, meaning it relies only on its structural strength to add stability to the shoulder. The labrum has no active defense against poor posture and dysfunctional shoulder mechanics. Prolonged poor posture and faulty moments of the shoulder complex are the number 1 killers of the labrum. Weakness in the rotator cuff can also potentially lead to labral tears. The rotator cuff muscles help position the shoulder into the socket and absorb shock when functioning effectively. A dysfunctional rotator cuff will cause an increase in stress on the passive labrum. The most common injury to the labrum is a “SLAP Tear”. The technical definition is not as important as understanding the mechanism of how a tear in such a thick and strong tissue like the labrum can occur. When the shoulder is placed in a position where the humerus is not centered in the joint socket, force is not transferred effectively to the rest of the body (a break in the kinetic chain). Any force applied to a poorly positioned arm is absorbed in the joint of the shoulder, partially in the area of the labrum where the shoulder is malpositioned. As we have discussed in the mechanisms of shoulder impingement, the head of the humerus bone tends to move up and forward in the socket when impingement occurs. The same is true of a SLAP tear, SLAP is an acronym that stands for "Superior Labral tear from Anterior to Posterior” (a tear in the top front part of the shoulder labrum). Labral tears can be the cause of pain in the shoulder at night, especially if a person is a side sleeper. If there is a tear in the labrum, there will be an obvious lack of passive stability. And because the individual is asleep, their active stabilizers (the muscles) are not functioning at 100%, making the shoulder unstable when pressure is applied. In an athlete with a labral issue, the pain reported in the shoulder is a dull pain, which can cause them to loose strength when preforming overhead movements. Depending on a patient’s athletic or lifestyle goals, surgery may or may not be indicated. Simply improving the individual’s posture, mobility, and stability can sometimes do wonders for even the nastiest SLAP tear. As I always tell my patients, if you are scheduled to pitch for the Yankees tomorrow, go talk to the surgeon. Otherwise, try a few week weeks of progressive rehab first!  Bicipital Tendonitis
As I discussed in part one of the shoulder blog, the long head of the bicep and its tendon act like the fifth rotator cuff muscle. The bicep tendon travels right next to the head of the humerus, where all of the other rotator cuff muscles attach. What is unique about the bicep tendon is that it travels through a grove in the shoulder bone called the bicepital groove, very similar to the patella (kneecap) and the patellar groove. In the knee, people are often diagnosed with “patellar tracking syndrome”, meaning the kneecap shifts to the side and rubs on the bones of the knee causing pain and discomfort. A very similar mechanism happens with bicep tendon in the shoulder. As the head of the humerus bone tends to move up and forward in the socket, as is common with an individual with impingement, a greater amount of stress is applied to the bicep tendon and it will become inflamed and painful. Think of the bicep as a long rubber band that runs from the elbow to shoulder blade. When the shoulder tilts forward and the head of the humerus travels anterior (forward), this add tension to the rubber band. Individuals with bicepital tendonitis usually have increase pain when they fully extend their arm and rotate. For example, turning a door knob is where the bicepital groove comes into play. Imagine again the very tight rubber band due to poor shoulder position, now when the arm is rotated, the bony ridges of the grove run into the rubber band (inflamed tendon) that no longer has any give or play because it was pretightened. If this tendonitis happens for a long period of time, months to years, the diagnosis changes to tendonosis, which we will discuss in a future blog post. It should be noted that in specific types of SLAP tears, the ligaments that hold the bicep tendon in the grove become torn as well. This can cause a slapping sensation in the shoulder when the bicep tendon literally pops out of the groove. The Silent Tear Tears in the rotator cuff actually occur quite frequently. The scary news is that many people have tears, and don’t realize it (asymptomatic). In the general population; Sher et al. took MRIs of 96 asymptomatic subjects, finding rotator cuff tears in 34% of cases, and 54% of those older than 60. This may be why it can take very little force to cause a tremendous amount of pain in a shoulder if there is already underlining damage to the shoulder. But, on a positive note, these silent tears prove that if the shoulder mechanics (posture, mobility, and stability) are functioning properly, an individual can go throughout life without having surgery and long recovery period. In part 3 of this shoulder blog we will talk about the 3 major components of healthy shoulder mechanics in more detail, they are posture, mobility, and stability.
0 Comments
Leave a Reply. |
AuthorDr. Chris Feil Archives
June 2024
Categories
All
|
 RSS Feed
RSS Feed