|
If the internet has done one thing for the world, it has made average people into “experts” on almost any topic with just a few clicks. My personal area of internet pseudo expertise is in the field of auto mechanics (just ask my wife how many times I’ve tried to save money fixing the car myself). It seems so easy on Youtube, and message boards always have creditable information, right? The same can be said for fitness and sport injuries information on the web. I believe the majority of content on the web is generally reliable (you are most likely reading this online), the problem starts when fundamentals are glossed over or basic concepts are assumed. In the world of functional exercise a great deal of attention is placed on athlete’s injuries, but not enough time and emphasis is spent on correct posture to prevent injuries. As fitness coaches and organizations push to continually challenge and vary workouts, one of the undervalued fundamentals of shoulder and spinal health, is the posture of the thoracic cage. I believe if coaches and athletes spent more time focusing on the posture and movement of the thoracic cage during exercise, several shoulder and spinal injuries could be prevented. Believe it or not, by simply observing the positioning (posture) of the thoracic cage prior to an individual preforming an exercise, you can estimate how successful they will be at performing the exercise.  My novice ability to fix a car is the perfect analogy as to why the position of the thoracic cage is so important during exercise. A few years back I needed new brake pads for my car, so I pulled up a trusty YouTube video, ordered my parts online, and took on the automotive challenge in the driveway of my new house. As I jacked up the car, I failed to notice that the driveway at our new house had a slight slope compared to our old driveway. Just as I removed the second front tire, the car began to slowly lean backwards. I jumped away as the car slipped off the car jack and crashed to the ground. In this analogy, the sloped driveway represents the thoracic cage, the jack represents the scapula (shoulder blade), and the car is the shoulder. In the rehab world, a great deal of emphasis is placed on “scapular stability” to help injured shoulders. I am here to tell you that scapular stability is functionally impossible to obtain if the thoracic cage is out of position. The bigger the slope in the driveway, the more unstable the car jack is! The thoracic cage consists of the spinal bones of the mid back (thoracic spine), the attaching ribs, and all of the muscles that attach to the bones and cartilage. The accepted term for faulty positioning of the thoracic cage is a “rib flare”. 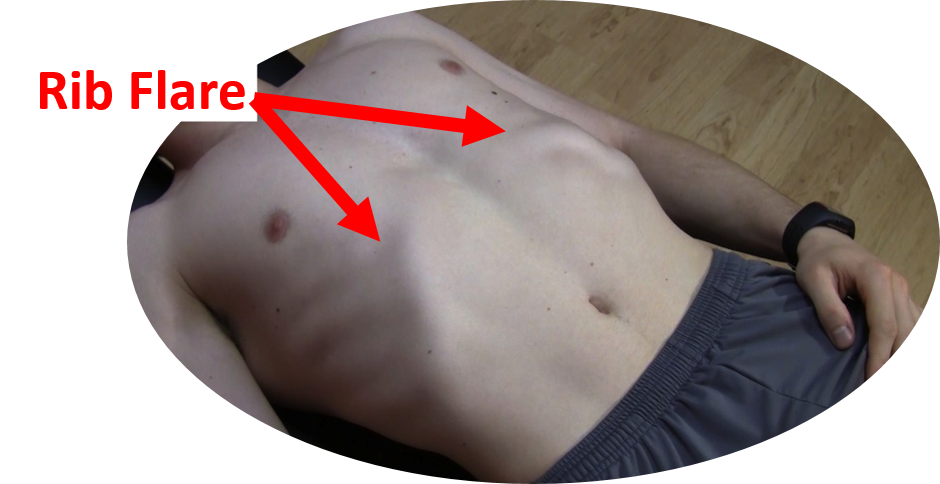 Picture taking a deep breath into your lungs and holding it, the resulting rib position would be an example of a rib flare. The entire ribcage is elevated and the base of the front of the rib cage is protrudes forward and out. Functionally this causes a lot of compromise in the body:
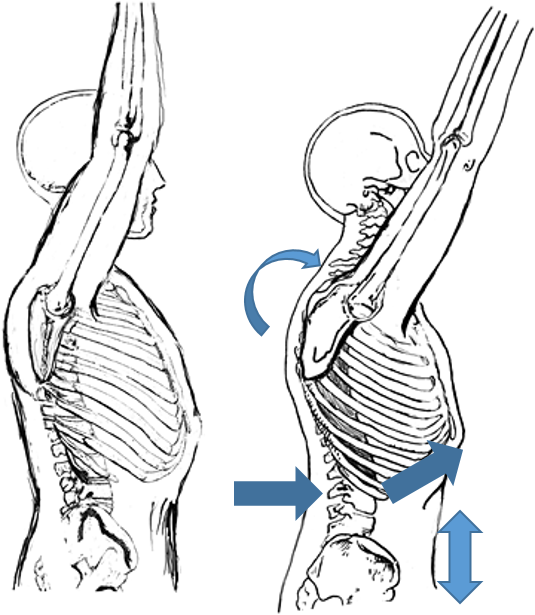 Why does a rib flare commonly occur in functional exercises like pull-ups, squats, push ups and overhead pressing? I think the number one reason people continue to exercise with a rib flare is that it provides “passive” stability when preforming explosive movements. “Active” stability is achieved by correct activation of stabilizing muscle groups in the region. For example, the abdominals and the muscles of the mid back. If the stabilizing muscle groups are inactive or weak, athletes will start to use the end range positions of their joints to provide a base of support for their body as they exercise. Meaning: the lower back joints lock into hyperextension and a rib flare causes the thoracic cage to become rigid and compressed, all to make up for a lack of active muscular stability. There are a few problems with this postural fault:
When I went back and re-watched the automotive Youtube videos after dropping my car, of course I saw there were blocks behind the tires when they jacked up their car. A slight detail that I originally overlooked. Now, anytime that I jack up the car, I place blocks under the tires to prevent the car from rolling down the driveway again. Going back to the shoulder analogy, the “tire blocks” represent our rotator cuff muscles. The number one job of the cuff muscles is to keep the shoulder stable in its socket. Athletes always ask me why their cuff muscles are tight and sore. I tell them it’s because of their posture; they usually give me a funny look. After a few visits they start to understand positioning the thoracic cage correctly during activity, enables the scapulae to stabilize in the thoracic wall, greatly reducing the stress in the lumbar spine and rotator cuffs. Correcting a rib flare may be as simple as tightening the core muscles to pull the rib cage back down prior to and during an exercise. But, in an athlete that has had a rib flare for several years, it may take longer to correct the problem. First they have to regain the mobility of the thoracic spine and rib cage. The best way to combat a long-term postural problem is a ton of foam rolling (don’t forget to roll out the ribs) and dynamic mobility exercises. The mobility exercises must be followed up with a retraining program targeting core/glute/ and scapular muscle activation and strength. Video analysis can be used to help the athlete visualize correct posture during exercise too. In summary- Strengthen your core and do more mobility work on your thoracic cage. Do not constantly hyperextend your lower back and flare your ribs when exercising Be sure to pay attention to details, and most importantly, never let me fix your car! By Dr. Chris Feil
9 Comments
 Over the last few weeks I've had several patients come in to Team Chiropractic and Rehab of Ames with calf strains. These people have hurt themselves running, golfing and kickboxing. All of these activities demand a lot of strength and explosive power from the lower body (yes golf is a lower body sport). It makes sense that an increased demand on the two muscles of the calf (gastrocnemius and soleus) would lead to a possible overuse and injury. Typically, a calf strain consists of a small portion of the muscle fibers tearing, resulting in a painful inflammatory reaction. At Team Chiro, we don’t just aid our patients in healing faster, we try to educate our patients on why their injury occurred and what they can do to prevent it from happening again. Functionally, I believe calf strains occur when there is a loss of motion in the ankle and/or a loss of functional gluteus strength. There are several reasons why modern man’s ankles become tight. First, most of us end up sitting in a desk /car all day, or we stand all day on flat hard surfaces. In both of these situations, the ankle is not challenged in all three plains of motion like it would be if we lived and worked all day on a primitive farm. As the old saying goes, “you use it, or you lose it”, well most us lose it when it relates to ankle mobility. Another common cause of lost ankle mobility is improper healing fallowing an ankle sprain. It is very common for the injured tissues of an ankle sprain to heal in a manner that restricts motion in the ankle if it is not properly rehabbed. (Hint: don’t just brace up a sprained ankle for a few weeks and call it good, get it checked out by a sports medicine professional.) When an ankle stops moving effectively, the muscles of the calf suffer. Say you lose 25% of your ankle range of motion, now physiologically the calf muscles begin to adapt to their new demands. The fibbers that help the muscle open up to it normal range of motion begin to contract over time. I use the analogy of some glue being spilled inside your muscle and hardening around the fibers that are no longer stretched due to the restricted ankle motion. Now, when this individual with the restricted ankle and compromised calf muscle tries to do something explosive like run up a hill, hit a golf ball out of the heavy ruff, or burnout on roundhouse kicks, their calf is setup to fail. The injury will occur when the muscle fibers of the calf that are doing all the work fatigue, or when the person puts the foot in a position where that lost 25% range of motion is needed and the weak contracted (glued) muscle are challenged.  Another interesting theory on why people strain their calf muscles is that the calf is compensating for weak glutes (your butt muscles). The human glutei muscles are the largest muscles in our bodies, yet many of us don’t use them effectively. Functionally, our glute muscles extend and rotate the hip/pelvis, propelling our bodies forward. Technically, our calf muscles can mimic the forward propulsion that the glutes perform, only from the ground up. But, that’s a lot of extra work placed on the calf, leading to overstrain and injury. It’s easy to visualize the mechanism of calf muscle compensation when you think of someone running up a hill without the ability to powerfully extend their hips. It’s harder to visualize the weak glutes and an overstrained calf in a golf swing or a roundhouse kick. The calf that typically gets overstrained is the rear leg in the golf swing and the calf in the kicking leg; it is actually compensating for the opposite side glute muscle weakness. Yes the opposite glute, if you are kicking with the right foot, the left hip/glute is where you start to generate all of the power for the right leg. When the left glute contracts it helps pull the pelvis and torso around, initiating a powerful impact with the bag. The calf injury will occur when the calf on the kicking leg pushes off the ground, trying to compensate for the weak pull of the opposite hip.  In golf, both glutes are important to a powerful efficient swing. On a right handed swing, the left glute will extend the pelvis, while the right will help with pelvic rotation on an explosive follow-through. If the glutes don’t activate the golfer will have a difficult time staying down on the ball (early extension); part of that problem starts in the calf musculature trying to excessively push the body off the ground to force the needed extension and rotation to swinging club.
The moral of this blog post is stretch your ankles and calf muscles, and don’t ignore your glute muscles when it comes to preventing future calf strains. If the glutes don’t contract, a person can compensate and try to generate all of the needed force from the calf to try to push the body into rotation and extension. Of course you can only do this so long before something breaks down! 
Believe it or not, when you were 10 months old, you probably had better push-up form/technique then you do now! How can that be? It’s actually quite simple, a healthy infant trains their stabilizing muscles all day long. They do this by the simple act of crawling. When you think about it, spending all day on your hands and knees does wonders for developing the muscles that run from your back and ribs to your shoulder blades (scapula), these muscles are what we in the rehab community call scapular stabilizers. Specifically, the scapular stabilizing muscles are: lower trapezius, serratus anterior, and rhomboids. Unfortunately these muscles are often underdeveloped and neglected.
As we get older, we tend to stop using the scapular stabilizing group of muscles in our modern lives. We spend hours sitting or standing with sometimes not so great posture. Even people that “go to the gym”, may not have an adequate ability to control their scapula because many of the exercises they preform are pushing exercises (there is a difference between a bench press and a push-up functionally). It is not coincidence that many of my patients that have shoulder pain and or neck pain/mid back, have tight chest muscles (Pec and Pec minor) and tight muscle that run from the neck to the shoulder (upper trapezius and levator scapula). Typically these muscles tighten because the scapular stabilizing muscles are under developed and under-utilized, leading to a rounding of the shoulders and an observable “winging” or elevation of the shoulder blades. Back to the baby push-ups to crawl effectively an infant must be able to keep their shoulder blades “glued” to their rib cage. This allows them to shift their body weight from one arm to the other as they pivot and crawl forward. Without this ability to stabilize their scapula, they would not be able to move from one arm to another while holding up their body. This concept of scapula hugging the rib cage is the big difference between a proper push-up and an exercise like a bench press. Bench pressing is grasping a weight and moving your hands up and down, actually the opposite motion of a push-up functionally. Preforming a proper push-up is really about using your shoulder blades to lift your torso up and down, much like the infant uses the shoulder blade to control the body while crawling. The concept may seem simple, but most people focus on their arms and hands too much when preforming push-ups and actually put their shoulders in a compromised position leading to increased strain on the shoulder and eventually impairment. Instead, focus on the tips below to help you revert back to your perfect baby style push-ups: · Start on the ground perfectly flat, lift the hands up of the ground and squeeze the shoulders blades down and back. (Keep the shoulder blades glued to the rib cages during the whole push-up movement) · Place the hands on the ground using a narrow hand position · Keep the hands below the plane of your shoulders · Direct the crease of your elbows forward (toward the direction of your head) as you push up · Shift the weight in your hands off the index finger and thumb to a more balanced palm pressure · Keep your pelvis and lower back in a neutral position · Keep your chin tucked in and your head retracted back.  Running is one of the most popular recreational sports in the United States. What I love about running is that it is a lifelong sport. Attend any local 5k race and you will see age ranges from 12 year olds to 80 year olds running the same race. It’s also a sport that doesn't require really fancy equipment to burn a lot of calories. (I have already discussed the main expense in running, shoes, in my previous blogs.) Another great thing about running is depending on your preference or your mood; you can run in groups or by yourself. With all of the great benefits of running, I find it interesting that runners rarely focus on technique or specific skill training for running. Maybe this is why over 1/2 of all runners injure themselves every year. At Team Chiropractic and Rehab of Ames, it is our goal to keep runners out of pain and prevent as many sports injuries as possible. It you want to become a good golfer, of course you would buy a set of clubs. But, often new golfers will pay for golf lessons. Actually, all ranges of golfers find it advantageous to hire a Pro to help them with their swing. Not only does coaching in golf make the golfer a better player, but it can help prevent injuries that occur with poor swing mechanics. For some reason, the idea of swing analysis for performance and injury prevention has not translated into the running community as much as the other recreational sports like golf. In this blog we will discuss one of the measurable aspects of the running gait, foot strike, and how effects performance and injury rate. (All of the information I’m going to share with you is very practical, however runners that have certain anatomical variances or injuries should consult a qualified health professional before trying to change their gait)  It All Starts At the Crash Zone: What I call the “crash zone” is the area of the foot that first contacts the ground while striding. The contact that a runner uses when their foot initially contacts the ground, determines their efficiency/speed, footwear selection, and their ability to absorb shock. Foot strike also directly relates to the susceptibly for most common running injuries: Shin Splints, Patellar tendonitis, IT Band Syndrome, Bursitis, Hamstring Tendonpathy, Plantar Fasciitis, Stress Fractures. There are basically three different ways to contact the ground when running:  Heel Strike- When the outside corner of the heel first impact the ground and then the foot rolls through to the mid and forefoot before toeing off. This type of impact mimics the foot contact while walking.  Midfoot Strike- When the first part of the foot that touches the ground is slightly behind the ball of the foot. After the initial contact, often the heel will briefly touch the ground before the gait cycle progresses to supination and the foot leaves the ground through toe off.  Forefoot strike- This is the classic “toe runner”. The first foot impact will be on or slightly in front of the ball of the foot. Rarely does the heel touch the ground with this type of running foot strike. Most sprinters use this contact; however there are people that use this type of contact to run long distances as well. Running with a Flat Tire:  Imagine if you raced two identical cars of the exact same year and model, but one car had a flat tire. It is quite easy to guess which car would win in this race. If you look at the picture of the flat tire below, you can see the large distance between the center of mass over the axil and the tipping point of the wheel. The greater the distance the more energy it requires to keep the wheel rotating. The same goes with running form. Runners who heel strike will have a foot impact at greater distance from their center of mass then an individual who impacts on their midfoot or forefoot. Most heel strikers are what we term “over striders”. Over striding puts them at a disadvantage biomechanically to preserve their momentum by reaching their leg out further from their body to heel strike (running with a flat tire).  It may seem mathematically advantageous for the heel striker with the long over stride when running long distances. The longer the stride, the less steps they need to take, right? Wrong, this is the most common amateur running mistake. Stride length is not as important as stride rate in any form of human running (sprinting or distance). Let’s do the math to prove this point: Assume that a 5 foot tall individual wants to run a mile. Typically your jogging stride length is just below your height. Studies show that the average stride length for armature runners is only 120 strides per minute (spm). - A typical heel striker runner runs at 120 spm x 4.5 foot stride = 540 feet per min (just under 10 min mile) - A heel strike runner who really over strides at 120spm x 5 foot stride= 600 feet per min (9 min mile) - A mid or forefoot striker who has a shorter stride but a faster cadence can do 160spm x 4 foot stride= 640 feet per min (8:15 mile) You can see that even with a much shorter stride length, the faster cadence or stride rate, ran much faster than even the supper over strider. By the way, 160 spm is a realistic goal for most recreational runners. An elite professional runner usually has a stride rate of 180-200 spm. Running with a Flat Tire While Stepping On the Breaks: Mathematically it should make sense why heel striking and over striding reduces running efficacy. But, anatomically and physiologically, heel strikers are at a disadvantage as well. By fully extending the leg to heel strike the runner does two things that put their bodies at a disadvantage (turn on the breaks). First, the extended heel striking leg has to fully lengthen the hamstring (the rear muscle to the leg). Weight lifters know that a long muscle is not a strong muscle. Running is all about elasticity in the muscle and tendons of the legs. When the muscle length is in a neutral position its tension to force relationship is at its maximum. However, when a hamstring is completely stretched out to because of the over striding, it loses a majority of its elastic springiness, leading to a slower cadence, more energy wasted by the muscle, and a decreased ability to absorb shock (can you say hamstring tear?). The second physiologic disadvantage of over striding is the body has to isolates muscle use. For example the quad (front leg muscle) has to fully contract to extend the leg fully to reach the heel contact. Verse in a midfoot strike the leg contacts the ground perpendicularly to the ground, letting both the hamstring and quad muscle function in a neutral length, which improves muscle elasticity and shock absorption. 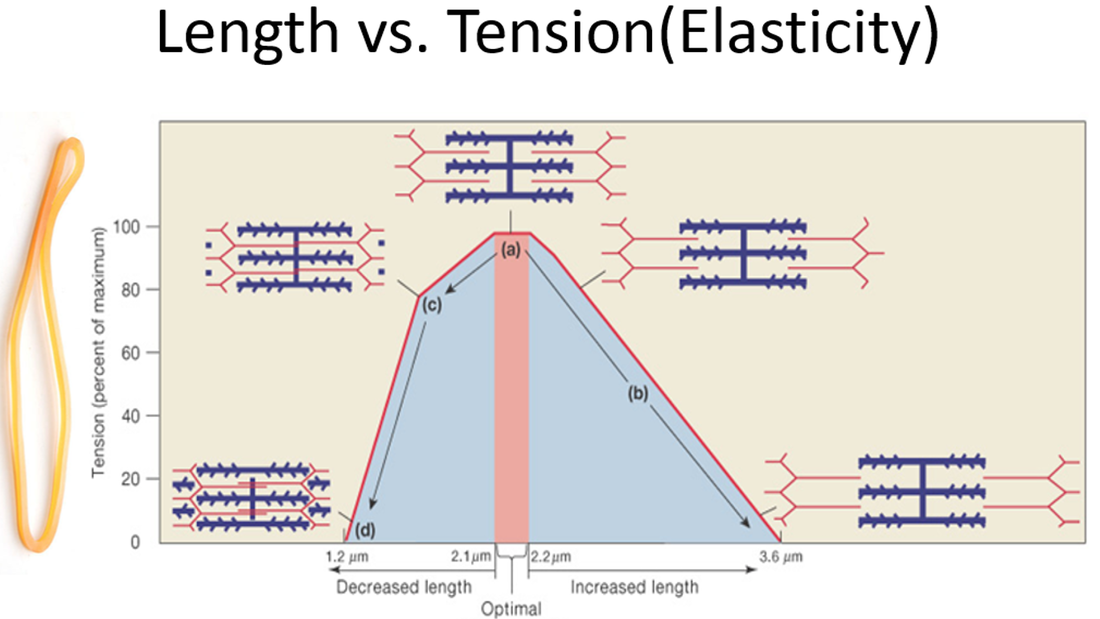 There is one other disadvantage biomechanically to heel striking while running. To get the foot in a position to heel strike, the body needs to move up and down vertically more to let the heel travel over the ground before striking. This is a big waste of energy and increases the ground impact force on every stride. Usually the objective with running is to use our energy to move forward, not up and down. The best graph to visually explain the differences in force transmission in different foot striking patterns is below. If you notice the one big difference in the parabolic arcs is the sharp initial peak formed when the heal striker first impacts the ground. Imagine the arc of the graph was that of path of a pebble that you toss to someone. On the curve of the midfoot striker the curve was very controlled and smooth, therefore the pebble would be easy to catch. Imagine on the heal strike graph that we took the pebble and placed it in a sling shot and then fired it. That increased rate of force at the impact of heel strike is like the pebble traveling at a much faster rate and can cause injury when trying to catch it. If the rate of the impact force is too fast, the human body cannot “catch” or absorb the forces effectively, meaning the bones, tendons, ligaments and muscles are susceptible to injury. 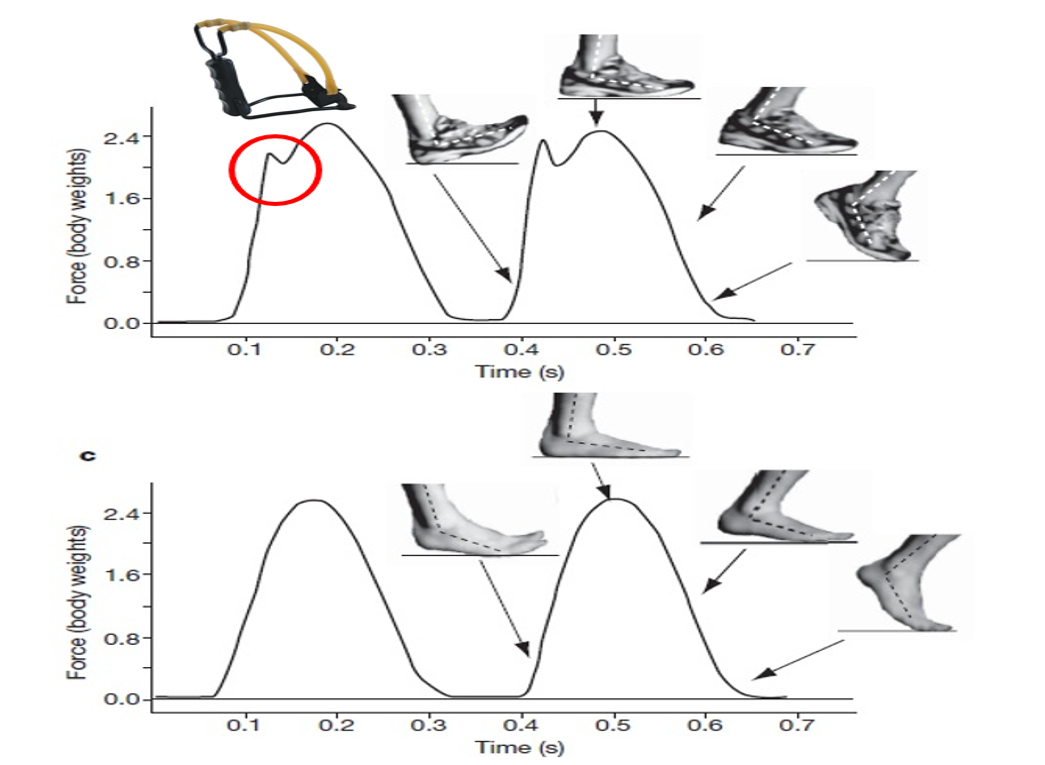 How Do Shoes Fit In? Because most recreational runners have been exposed to high drop running shoes their whole lives, we have tricked our bodies into thinking it’s OK to hit the ground with our heels while running. I have discussed the reasons for this in my previous blogs on minimalist shoes and shoe fitting. It’s interesting how humans have been running for millions of years, yet within a few decades of wearing athletic shoes, many of us have completely forgotten how to run effectively and safely. If you want to make a change to running on your mid foot, find a shoe with a lower drop and a wide toe box to let your foot expand when running. However I do caution you that changing to a zero drop shoe “cold turkey” can be dangerous. Give your body time to transition to a new shoe, vary the shoes over the week and start with a hybrid shoe first before a full zero drop shoe. What about Forefoot Running: As I mentioned earlier, forefoot running is mostly done in sprinting. Running on the forefoot does lead to faster stride rates, but there are some distinct disadvantages to forefoot running for a long distance. First, just like heel striking, forefoot striking causes muscle to work in isolation and in shortened or elongated states. Forefoot strikers often have injury problems with their calf muscles because they have to contract and shorten during most of their gait cycles, leading to strains, tears and Achilles injuries. Also landing on the forefoot is not as stable as a midfoot strike (imagine running in high heel shoes). This instability will put the tendon and ligaments at risk (ankle sprains and Achilles tendonitis). Finally and not a big surprise, toe runners will have issues with stress fractures and injuries to their toes, the function of the four smaller toes is to help with balance, not to absorb shock on impact. How to Make a Foot Strike Change: Changing your gate is like learning to write with your non-dominant hand. You may have spent years running with a heel strike, it is imposable to change that overnight. I suggest a transition period of 2-3 months to make a gate change. First it take muscles several week to change in length, you can only expect injuries if you don’t let your body slowly adapt to the new running technique. Next there is the mental aspect of changing your form. Most people like to run because it lets them turn off their minds and relax. When you try to change your gait, you have to be consciously aware of every new movement your body makes. It will again take several weeks for this new running form to become reflexive or unconscious. I suggest in the beginning of the transformation, you only focus on form and technique for 1-2 minute periods during your run. For example after every mile, you focus on technique for an 1/8th of the next mile. Making the change to a midfoot strike is well worth the effort, you will be less susceptible to injury, and be a more efficient and faster runner!  Now, for the blog that everyone really wants to read, let’s talk about running shoes. In part 1 of the blog we thoroughly broke down the human foot and laid the foundation of how to evaluate your foot before buying a shoe. Now we need to look at the different parts of a shoe and how shoes can affect the way your foot functions. Hopefully, this blog will be able to streamline the elements of the shoe that really matter, and show you what aspects of a shoe don’t really matter and are just “Shoe Bling”. I want to thank JAX Outdoors for letting me use their shoes as demos in my community presentations and take pictures of them for this blog. If you have never been to JAX, it’s worth a trip to west Ames to check them out for any of your sporting good needs. When shopping for shoes, you need to have plan for finding the shoe that fits your needs as runner anatomically and functionally (learn more about your foot anatomy and biomechanics in Part 1). For example a runner with a mid-foot strike pattern with a history of ankle sprains that runs daily on cement needs different shoes then a person that only runs on tails, heel strikes, and under pronates. You always need to remember when shopping for shoes, that shoes are tools. Tools help us accomplish tasks more efficiently and help take stress off our bodies; shoes are the same way. But, when all you have is a hammer, and you need a screwdriver, problems will arise. In shoes, the wrong type of shoe can cause injuries and poor fitting shoes will wear out faster too. Shoes can also be used as tools to help change running technique or help protect an injury while it heals. 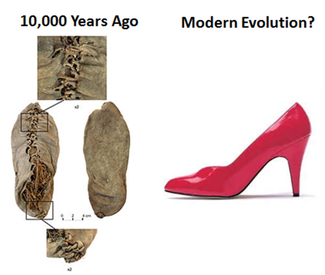 Shoe History: Humans have been walking on two feet for over 5 million years, but the earliest evidence of shoes only carbon dates back 10,000 years. Back then, primitive shoes where were worn to cover and insulate the feet from the elements. Athletic shoes have a very short history, about 100 years ago with development of rubber; companies like Goodyear started producing “sneakers”. It was not until 1970 that Phil Knight and Bill Bowerman began experimenting by pouring liquid rubber onto a waffle iron, that the modern day running shoe was developed. http://www.holabirdsports.com/running-tech-center/running-shoe-history.html Runners typically seem to develop a brand loyalty with shoe companies. Unfortunately this loyalty will get the runner into trouble eventually. Running shoe company's top engineers and executives are like NFL coaches. It seems like every year, half the NFL teams switch coaches and very few coaches now days spend their entire career with one team. The same thing is going on in the running shoe industry. If some new engineer comes up with a new shoe design for company X, Company Y will give the engineer a pay raise to quit and work for them and bring the new knowledge. So when this hot shot engineer takes his new job, he is going to change the design of your favorite shoe from company Y. If the companies are not loyal to you the consumer, you shouldn’t be loyal to them, just find the shoe that fits. Another little corporate secret is that most companies only use about 3 different molds to manufacture all of their shoes. Meaning, you are paying extra money for bright colors and “shoe bling” on shoes that have the exact same midsole and outer as the less expensive models. 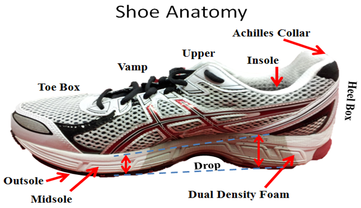 Shoe Anatomy: Starting from the ground up, the part of the shoe that actually contacts the ground is the outsole and is made from a strong dense material. The next layer is the midsole and most of the flexibility and control of foot motion is controlled with in this layer. Typically it is formed from foam, many times different densities and stiffness of foam are used in areas of the shoe where motion of the foot needs to be slowed down. This is called a shoe with dual densities, there may be more than just two types of foam depending how much stability is needed. The layer contacting the foot is the insole, many times this is replaced by an insert or orthotic. An orthotic or athletic insert usually has some type of posting. A posting is anything (foam or plastic) that tries to limit pronation of the foot. Finally, there are the parts of the upper including the heal box, vamp, and toe box. An important measurement that should be addressed in all running shoes is the “drop”. Shoe drop is the delta or change in height from where the forefoot and mid foot are positioned off the ground compared to the rear foot. There are three basic types of shoes. Each one is designed for an ideal category of foot type. As we explained in Part 1, rarely does the shape of the foot (flat, neutral, high arched) match the actual function of the foot (over-pronated, neutral, and under-pronated). But, shoes are still basically broken down into 3 categories matching the 3 foot types: Cushion Shoes, Stability or Neutral Shoes, and Motion control Shoes. I will add four more categories to this discussion, they are: Minimalist, Hybrid, Toe spring, and Trail running shoes.  Cushion Shoe: -Purpose is to absorb large amounts of shock while not limiting foot movement. -Designed for the runner who under pronates. -Typically an under-pronator has a stiff foot, so they need a flexible shoe (many times there will be a break in the midsole between the rear foot and forefoot to promote increased shoe flexibility). -Have a curved sole to fit a high arched foot.  Neutral or Stability Shoe: -Propose to provide shock absorption and basic stability. -Designed for the ideal foot, or a person who wears orthotics. -A semi curved sole with moderate flexibility. -Theoretically, the most purchased running shoe.  Motion Control Shoe: Propose is to provide maximum stability and support of the foot that over pronates. Very dense, heavy, and thick foam is used in the midsole. The sole is almost straight and there is minimal motion when the shoe is twisted. (It should be noted that in several studies, every classification of runner who ran in motion controlled shoes had increased injury rates compared to other types of running shoe test. Please don’t release the Brooks Beast.) 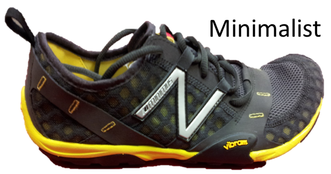 Minimalist Shoe: The purpose is to mimic barefoot running while still protecting the foot from the elements. Extremely lightweight, minimal to zero drop, maximum flexibility, and a large toe box or individual toe capsules. (You can read more about minimalist shoes in my previous blog)  Hybrid: Purpose is to bridge the gap between a cushion shoe and a minimalist shoe. A small drop, and high flexibility, light weight, while still providing some shock absorption. Example: Nike Free 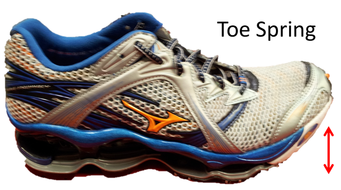 Toe Spring: Purpose is to provide artificial big toe flexion and ankle dorsiflexion for individuals who lack those ranges of motion. A stiff sole with a large arched relief under the forefoot to rock over during gait.  Trail Running shoe: Purpose is to provide a light weight traction shoe that limits ankle sprains. Bottom treads that wick away mud, yet provide superior traction. A low drop with a wide heel to reduce the severity of ankle sprains. Women’s Shoes: There are more than just color differences between male and female shoes. Anatomically and biomechanically, there are significant differences between men and women. Women have shorter legs (as a ratio of total height), wider hips, and more valgus alignment of the knees (“knock knees” or higher “Q” angle). When it comes to shoe fitting they often have more trouble finding shoes that fit well than their male counterparts. Women have triangular and narrower feet compared to males who have more square and wide feet. Their malleoli (ankle bones) are also lower. Women are also more likely to develop foot deformities such as bunions and need to be fit for shoes that provide adequate toe box room. Recommendations for Mid foot and Forefoot Strikers: I recommend a forefoot or mid foot striker wear a shoe with very little drop. Because a high heel/large drop shoe will cause a premature heel strike. This type of runner doesn't need excessive heel cushioning/motion control features, because pronation and shock absorption is basically over when their heel hits the ground. They are often better off with a hybrid or minimalist shoe style. These shoes offer adequate room in the toe box for increased widening of the forefoot on initial contact. If possible a flared heel cuff can be used to add support of the rear of the shoe during contact, taking strain off the Achilles tendon.  In the Shoe Store Tips · Weight it: heavy shoes usually provide more shock absorption and/or motion control, but they add weight that must be moved in every stride. · Twist it: does the mid foot flexibility match your foot type needs? · Bend it: does the forefoot bend where your big toe joint is placed within the shoe? · Poke it: are there dual density foams in the right areas for your needs? · Look at it: what is the curve in the sole like? How much of the shoe is “bling”? · Bring the socks you generally wear running to use while trying on the shoes. · Try on shoes later in the day or right after a run so your feet will have swelled. · Shoes should feel great when you put them on, don't buy them thinking you will "wear them in." · If you have wide or narrow feet, look for a brand that has multiple widths to fit your feet. · Find a different shoe if any part of your foot feels like it is rubbing · Do not shop when you are in a hurry. Be sure to walk/run around the store for a few minutes on a hard surface. · NEVER buy “seconds” shoes online, these shoes may save you $20 initially, but in the long term they can cost you much more if you are injured. The reason many shoes are sold at a discount online is that there is a manufacturing flaw within the shoe. Would you by a powertool or a car that had a mechanical defect? (In part 3, the last of the Shoes 101 blog, there will be a discussion about the cause of different running injuries and different shoe strategies to help heel and prevent future injuries) The goal of these next blog posts is to remove some of the mystery of how to find the right running shoe for your specific foot. For the average consumer, shopping for a good pair of running shoes can be daunting. There are thousands of different models and styles of shoes to pick from. It doesn’t help that most costumers are influenced more by TV commercials about the shoe and how the shoe looks esthetically, than how it actually functions on their foot. I like to use the analogy that shopping for running shoes is like buying a $100 lotto ticket. It’s exciting when you are purchasing the ticket, but there is often buyer remorse when you get home and you realize the ticket was not a winner. Even more frustrating if you do find a winning ticket, you can never play the same numbers again because the shoe companies are always changing their shoe designs. Hopefully, after reading this blog, you stop feeling like you’re always playing the lotto at the shoe store, and your shoes always feel like a million dollars!   This blog will be 3 parts long. It will start by discussing what goes into a shoe first, that being your foot. The shoe must match your foot, not the other way around. Then in the second part, it will breakdown shoe anatomy and the different types of shoes and how they can help improve function and decreases injuries in runners. There will be a brief discussion in this part on running style/technique and the type of shoe that suits the runner (I will post more specific blogs on running form and technique in the future). Finally in the third part, I’ll post about several injuries that occur while running and how to prevent and aid in healing specific injuries with specific shoes. Getting to know your own Foot: Humans started to walk bipedal (on two feet) anywhere from 5 million to 10 million years ago, depending on which archeologist you ask. The transition from ambulating on all fours to bipedalism may actually have been one of the most important evolutionary developments in mankind. There are two theories on why we started to walk up right. The first is that by walking only on our feet, we freed up our hands to use tools. The second idea, and most accepted theory is that by walking on two feet, human beings became more efficient. Ancient humans were able to walk/run for greater distances; which improved their ability to hunt. Bipedal man could literally chase his pray to death because of the improved efficiency. Maybe this why modern man still has the deep desire and love for running long distances?  To make the physiological change to bipedal locomotion, some major adaptions had to take place in the human body. First our posture changed to a more vertically erect posture, we developed a lumbar lordosis/mobile lumbar spine. The shape of our pelvis changed and many of the muscle of our pelvis had to change their function compared to other primates. I believe this is why so many injuries can be related back todysfunctional hips in modern man. Finally, our feet had to change in shape and function. We ask more out of our feet than any other animal on this planet. Our feet act as a stable platform for when we need to stand for hours, they act as the first line of shock absorption and they also transform into ridged levers when we need to push off in running. The human foot is composed or 33 different joints and 26 bones. The structure of the foot articulations give the foot the ability to be very mobile and then stiffen depending on the position and contraction of muscles. Speaking of muscles, there are two types of muscles that attach to the foot, a short group called the “intrinsics”that are found within the foot, and then there are longer muscles that start at the leg bones (tibia/fibula) and then attach to the bones in the foot. The muscles and ligaments hold together the arches of the foot. Yes, I wrote arches, with an “s”. There are actually three different arches in the foot, the medial arch that most people think of when they think of a foot arch runs between the base of the big toe to the inner heel. The longitudinal arch runs along the outside of the foot, and the transverse arch runs across the forefoot. Together, these arches create a triangle or tripod within the foot. It doesn’t matter if you have really high arches or a “flat” foot; everyone needs to support themselves on the three points of the foot tripod. The most common deformity that occurs when there is a dysfunctional foot tripod is a bunion. When the tripod point at the base of the big toe becomes dysfunctional, the angle of progression changes when you walk (over pronation), forces are distributed unevenly, and muscles that usually anchored from that tripods point become weak. If this occurs over several years, the forefoot will widen and the joint of the big toe with start to deform.   As I mentioned previously, the foot needs to be a mobile shock absorber, for 5 million years humans walked barefoot on uneven terrain (it was not until the last few hundred years that humankind made everything flat with cement and concrete). This ability to keep the joints of the foot loose and adaptable is termed “pronation”. Pronation gets a bad rap; really, it is one of the most important motions in your foot. As a runner I would take a foot that slightly over pronates any day over a foot that doesn’t pronate enough. The motion of pronation is complicated when you breakdown the motion of every bone in the foot, but for the sake of simplicity, think of pronation as the foot “collapsing or rolling in”. Supination is the exact opposite of pronation, it is the mechanism of making the foot a “ridged lever”. As we walk or run, after we have adapted to the ground, absorbed the shock of impact through pronation, we transfer our body weight over and past our foot by pushing off through supination. It would not be very efficient to push off if the foot was still a “loose bag of bones” as it is in pronation. During supination, the muscles and tendons of the foot and leg bring the foot downward and inward, causing the bones of the foot to lock (windlass effect).  Some rights reserved by sportEX journals Some rights reserved by sportEX journals Bio-mechanically, there are differences between running and walking. Walking can be described as a pendulum motion, where the rotation of the different parts of the body preserves momentum. In walking, the foot is in contact with the ground 60% of the time, and both feet are touching the ground simultaneously at different parts of the walking gait cycle to preserve the momentum used to propel walkers. Running uses principles more related to a spring. Running relies on the elasticity of the muscles and tendons to propel the runner forward. In contrast to walking, most of running is done in the air (40% foot ground contact time) and only one foot is ever in contact with the ground at one time. During running, pronation occurs during 70% of the ground contact period, and supination comprises the rest of the time the foot touches the ground. So what’s the big deal about “over pronation”? As stated previously, pronation is essential to human movement and actually helps prevent injuries then it causes. But, when pronation occurs at a speed or rate that your body can’t control, you can have complications that lead to injuries and decreased performance. I use a slingshot analogy to explain the concept of over pronation. I can pick up a pebble and toss it to someone; they will be able to catch it without difficulty because of the predicable slow speed of the toss. However, if I take that pebble and load it into a slingshot and fire it at someone, they will not be able to control and stop the pebble without some type of shield, or they will become injured. The shield in this analogy is a shoe or an orthotic that slows down the pronation. The worse type of over pronation is one that only happens in one foot, and not the other. In this case there is an asymmetry in the body that travels up the kinetic chain. (over pronation causes the lower leg to rotate in, the knee to twist down and in, the thigh rotate causing the pelvis to tip down and forward, leading to a curve in the lower back and a compensation in the middle back, dropping and rounding one of a shoulders).  Some rights reserved by whiteafrican(flicker) Some rights reserved by whiteafrican(flicker) So what’s the big deal about “over pronation”? As stated previously, pronation is essential to human movement and actually helps prevent injuries then it causes. But, when pronation occurs at a speed or rate that your body can’t control, you can have complications that lead to injuries and decreased performance. I use a slingshot analogy to explain the concept of over pronation. I can pick up a pebble and toss it to someone; they will be able to catch it without difficulty because of the predicable slow speed of the toss. However, if I take that pebble and load it into a slingshot and fire it at someone, they will not be able to control and stop the pebble without some type of shield, or they will become injured. The shield in this analogy is a shoe or an orthotic that slows down the pronation. The worse type of over pronation is one that only happens in one foot, and not the other. In this case there is an asymmetry in the body that travels up the kinetic chain. The best story of this relationship between the foot and rest of the body comes from baseball. In 1937, Dizzy Dean was pitching in an All-Star game. The batter hit a comebacker that hit Dean’s foot, fracturing his toe. While still nursing a sore foot, Dean resumed pitching. The soreness caused him to change his foot position and his pitching mechanics, leading to shoulder and arm problems. Dean was never able to overcome his shoulder injury, leading to his early retirement. His quote ““Fractured. Hell, the damn thing’s broken!”. 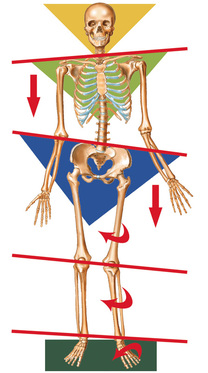 over pronation causes the lower leg to rotate in, the knee to twist down and in, the thigh rotate causing the pelvis to tip down and forward, leading to a curve in the lower back and a compensation in the middle back, dropping and rounding one of a shoulders (image produced by footlevelers) Is There an Ideal Foot? Many people make the mistake of only looking at their foot when are trying to determine if they under or over pronate. The assumption is that if your foot is “flat” you must over pronate. This is a myth, if a person with a flat foot uses their foot tripod effectively, they may not have a pronation problem at all. Actually, a person with a flat foot can have a very stiff and ridged foot and may need a completely different type of shoe compared to what it looks like they should wear. The best example of this is the fastest man in world, Usain Bolt. Did you know he has flat feet? I don’t think I remember watching him run at the Olympics in heavy motion control shoes. Sadly many people with flat feet with normal foot mechanics are improperly fit into a motion control shoe or an orthotic. This causes them to complain the shoes are uncomfortable due to the artificial arch that presses into their underfoot. Actually, people with high arches that have very mobile and loose feet are more likely to become injured because their body can’t control the rate in which their foot collapses at a greater distance because of their high arch starting point. 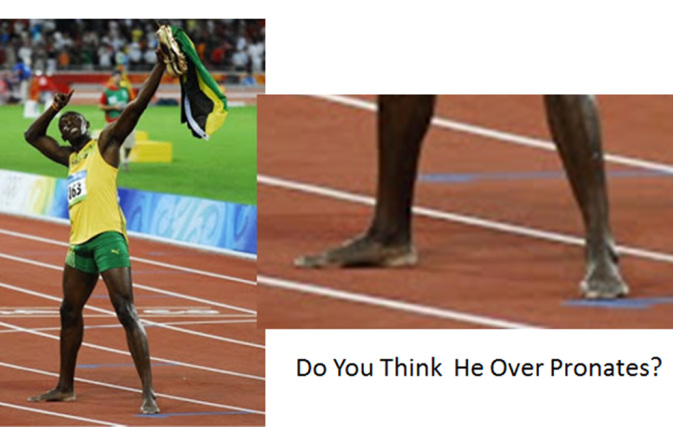  Image from www.dukehealth.org Image from www.dukehealth.org Much like the stereotyping of flat feet, there is an assumption that people with high arches need a cushion shoe because it is assumed that their foot is very stiff and they supinate more than they should. And the person with a “normal” looking arched feet (what ever normal is?) should be ok in a stability/neutral shoe. The moral of the story here is that looks can be deceiving. I can look at a door and assume I know how it moves, but until I physically open it, I never know if the door moves easily or is locked/jammed. The best way to tell how a foot moves is to have a professional palpate the motion of a foot and then analysis the foot when walking/running. Palpating your own foot or trying to self-analysis your gait can be tricky. The easiest way to tell about your foot tendencies during your gait cycle is to look at the wear pattern of an old pair of shoes. I call this “arch”eology (sorry it’s a lame pun). The two other variables in foot function that become very important when fitting shoes are: 1. Where and how much your big toe bends in relation to the shoe. You may have never realized the ramifications that people have different sized toes, and the joints of the toes don’t always match where the shoe bends (can you say turftoe?). Typically in an athlete the big toe should bend up in the air 65 degrees when standing flat. There is also specific group of people that have a Morton’s foot, this is easy to distinguish because in a Morton’s foot the 2nd and maybe 3rd toes are longer then the first toe. This causes an alteration in toe off when they run and special attention needs to be paid in fitting them into a shoe that bends in the forefoot at the proper location. 2. How well your ankle flexes (dorisflexs) is also really, really, really important in runners and all other athletes. The number one reason we lose our ability to flex our feet are ankle sprains. If you severely sprain your ankle and never properly rehab after, the ligaments on the side and back of the foot scar down and you end up losing the ability to flex the ankle. In a runner ankle dorsiflexion should be between 20 and 30 degrees. Anything less will shorten the stride length and put excess stress on the soft tissues of the plantar fascia, Achilles tendon and the calf musculature.   The last point I’ll make before we start to break down shoes in the next blog, is that there are these things called legs that attach to your feet. In an ideal world there would never be anything wrong with the legs above the feet that could cause concern about shoe fit and function. But, we live in the real world, not an ideal world. For example, if people have knees that are bowed out or knocked in, special consideration needs to be made in shoe choice. Sometimes function may call for one type of shoe, but that shoe will not work with the individual because the shoe makes a condition in the knees or hip/back worse. This is when compensation needs to be made in shoe choice and professional help should be sought out.  Supraspinatus moving under the bony arch of the scapula Common Shoulder Pains/ Injuries: Because of the tremendous range of motion required by the shoulder to preform functional everyday tasks or recreational activities, the shoulder is highly susceptible to injury. The shoulder becomes most susceptible to repetitive injury when lifting items or when the arm is placed in an overhead position. To perform these motions without injury requires unabated shoulder range of motion and optimum shoulder stability. It does not matter how “strong” your shoulder is when posture and scapular range of motion are limited, there will be a stronger potential for shoulder injuries. Below is a list of many common injuries to the shoulder. (Note- laxity and dislocations will not be addressed in this blog post) All of these injuries occur with a similar mechanical injury mechanisms and underlying causes: Impingement: A very common injury of the shoulder is what is termed as impingement. Just like the name implies, impingement of the rotator cuff muscle (supraspinatus specifically) develops when the space between the rigid coracoacromial arch (top of the shoulder blade) and the head of the humerus (arm bone) narrows. The muscles and tendons of the rotor cuff that pass through this space begin to fray and eventually may tear because they are pinched between these hard surfaces. Why does this space narrow? Anatomically, it narrows due to bony spurs, degenerative changes, or soft-tissue thickening. Functionally, the space narrows due to dysfunctional synchronicity of the rotator cuff muscles, aberrant scapular-humeral rhythm, or faulty scapular positioning during overhead arm movements. Individuals who are predisposed to impingement have several traits that can be distinguishable by even the untrained eye. First and foremost, a susceptible person’s shoulders commonly have the appearance of being rolled forward. Everyone has seen this person before in the local gym, their workouts consists of bench pressing and more bench pressing. They look great from the front, but when you look from the side, their shoulders sickout in front of their body. Anatomically, the scapula has tipped forward and the humerus no longer sits centered in the socket of the shoulder joint. Because the head of the humerus is positioned more forward and superior in position, the individual becomes more susceptible to impingement. These postural changes lead to the described narrowing of the space for the tendons of the rotator cuff, and start the impingement process. Typically, this postural fault of the shoulder stems from tightness and shorting of the chest muscles(Pec Minor) and reciprocated weakness and lengthening of the scapular muscles that normally stabilize the scapula to the ribcage. Interestingly, almost all cadaver studies show at least some type of fraying of tendons due to impingement. Some fraying is normal over a lifetime, but many people speed this process due to poor shoulder function, leading to actual tears in the rotator cuff muscles. A full tear of a rotator cuff muscle or tendon can cause full loss of strength in specific movements and may need to be surgically fixed. 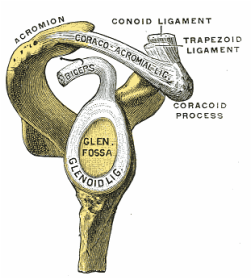 The Labrum= Glenoid Lig Bursitis In a majority of shoulder impingement cases, there is some form of bursitis involvement. Bursas are fluid filled sacs that are located throughout the body in areas of stress. They act like little pillows or shock absorbers. Most commonly they are located where a tendon travels near a bone. For example there is a bursa that is under the patellar tendon of the knee and it protects the tendon from friction with the tibia (leg bone) as it moves. There is a bursa positioned directly above the tendons of the rotator cuff in the shoulder, the “sub-acromia bursa”. When the mechanisms of impingement occur and the anatomical space narrows between the head of the humerus and scapula, not only does the tendon start to fray, but the bursa in this space is irritated. An irritated bursa will lead to an inflamed and painful bursa. When the shoulder bursa becomes inflamed, it will swell up causing even more compromise to the canal space. Many times medical doctors will inject this bursa with an anti-inflammatory to reduce the pain and swelling. But, until the mechanical stress is removed from the bursa, it will continue to become more inflamed in the future. Labral Tear - SLAP Tear The labrum gets its name from the world of architecture. In Roman architecture, a labrum was a large water-filled vessel or basin with an overhanging lip. This is actually an accurate definition of the labrum in the human shoulder. The human labrum is a layer of fibrous cartilage that surrounds the socket of bone on the scapula where the arm meets to form that shoulder joint. Because the bony socket is very shallow, the labrum adds extra depth to the socket, keeping the shoulder joint more centrated. Just like in Roman architecture, the labrum has an overhanging lip that extends around the ball head of the shoulder. The labrum in the shoulder is what we refer to as a “passive stabilizer”, meaning it relies only on its structural strength to add stability to the shoulder. The labrum has no active defense against poor posture and dysfunctional shoulder mechanics. Prolonged poor posture and faulty moments of the shoulder complex are the number 1 killers of the labrum. Weakness in the rotator cuff can also potentially lead to labral tears. The rotator cuff muscles help position the shoulder into the socket and absorb shock when functioning effectively. A dysfunctional rotator cuff will cause an increase in stress on the passive labrum. The most common injury to the labrum is a “SLAP Tear”. The technical definition is not as important as understanding the mechanism of how a tear in such a thick and strong tissue like the labrum can occur. When the shoulder is placed in a position where the humerus is not centered in the joint socket, force is not transferred effectively to the rest of the body (a break in the kinetic chain). Any force applied to a poorly positioned arm is absorbed in the joint of the shoulder, partially in the area of the labrum where the shoulder is malpositioned. As we have discussed in the mechanisms of shoulder impingement, the head of the humerus bone tends to move up and forward in the socket when impingement occurs. The same is true of a SLAP tear, SLAP is an acronym that stands for "Superior Labral tear from Anterior to Posterior” (a tear in the top front part of the shoulder labrum). Labral tears can be the cause of pain in the shoulder at night, especially if a person is a side sleeper. If there is a tear in the labrum, there will be an obvious lack of passive stability. And because the individual is asleep, their active stabilizers (the muscles) are not functioning at 100%, making the shoulder unstable when pressure is applied. In an athlete with a labral issue, the pain reported in the shoulder is a dull pain, which can cause them to loose strength when preforming overhead movements. Depending on a patient’s athletic or lifestyle goals, surgery may or may not be indicated. Simply improving the individual’s posture, mobility, and stability can sometimes do wonders for even the nastiest SLAP tear. As I always tell my patients, if you are scheduled to pitch for the Yankees tomorrow, go talk to the surgeon. Otherwise, try a few week weeks of progressive rehab first!  Bicipital Tendonitis
As I discussed in part one of the shoulder blog, the long head of the bicep and its tendon act like the fifth rotator cuff muscle. The bicep tendon travels right next to the head of the humerus, where all of the other rotator cuff muscles attach. What is unique about the bicep tendon is that it travels through a grove in the shoulder bone called the bicepital groove, very similar to the patella (kneecap) and the patellar groove. In the knee, people are often diagnosed with “patellar tracking syndrome”, meaning the kneecap shifts to the side and rubs on the bones of the knee causing pain and discomfort. A very similar mechanism happens with bicep tendon in the shoulder. As the head of the humerus bone tends to move up and forward in the socket, as is common with an individual with impingement, a greater amount of stress is applied to the bicep tendon and it will become inflamed and painful. Think of the bicep as a long rubber band that runs from the elbow to shoulder blade. When the shoulder tilts forward and the head of the humerus travels anterior (forward), this add tension to the rubber band. Individuals with bicepital tendonitis usually have increase pain when they fully extend their arm and rotate. For example, turning a door knob is where the bicepital groove comes into play. Imagine again the very tight rubber band due to poor shoulder position, now when the arm is rotated, the bony ridges of the grove run into the rubber band (inflamed tendon) that no longer has any give or play because it was pretightened. If this tendonitis happens for a long period of time, months to years, the diagnosis changes to tendonosis, which we will discuss in a future blog post. It should be noted that in specific types of SLAP tears, the ligaments that hold the bicep tendon in the grove become torn as well. This can cause a slapping sensation in the shoulder when the bicep tendon literally pops out of the groove. The Silent Tear Tears in the rotator cuff actually occur quite frequently. The scary news is that many people have tears, and don’t realize it (asymptomatic). In the general population; Sher et al. took MRIs of 96 asymptomatic subjects, finding rotator cuff tears in 34% of cases, and 54% of those older than 60. This may be why it can take very little force to cause a tremendous amount of pain in a shoulder if there is already underlining damage to the shoulder. But, on a positive note, these silent tears prove that if the shoulder mechanics (posture, mobility, and stability) are functioning properly, an individual can go throughout life without having surgery and long recovery period. In part 3 of this shoulder blog we will talk about the 3 major components of healthy shoulder mechanics in more detail, they are posture, mobility, and stability. By Dr. Chris Feil, Team Chiropractic and Rehabilitation of Ames It has always puzzled me why when we sit at work all day, why people want to go to the gym and sit more while they work out? The concept of functional exercise has turned that idea of static isolated exercise upside down! Functional Exercises principles focus on building a body capable of doing real-life activities in real-life positions, not just lifting a certain amount of weight in a static posture created by a gym machine. Functional exercises tend to be multi-joint and multi-muscle exercises, or what we call compound movements. Instead of only moving the elbows, for example, a functional exercise might involve the elbows, shoulders, spine, hips, knees and ankles. Not only is functional exercise fun, because you are up moving around, you also get the benefit of exercising at higher intensities because you are using all the muscles in your body during the whole workout. The more muscles you use, the more calories you burn! Also, by performing exercises like kettelbells and kickboxing that use several muscles groups, you start to train the neglected areas of your body, without even thinking about it. Neglected areas, like your middle back, hips, abdominals, and even your feet. When these areas are strong, they help prevent injuries and make exercise and your everyday activities easer. Where did the Traditional American Gyms Go Wrong? Today traditional American gym workouts often focus on isolating and challenging one specific muscle. Usually, one movement of a joint is preformed in a controlled range of motion, while the rest of your body’s muscles remain static and dormant. This mindset comes from the body building culture. When Arnold Schwarzenegger needed to tone each individual muscle, he and his friends devised sets of specific exercise to make their muscles "bulge" when he flexed on stage or in the movies. There are several problems with that approach; traditionally bodybuilding overdevelops certain muscles, like the chest muscles, biceps and quads. When these muscle groups become too strong and out of balance with the rest of our bodies, they pull our posture out of alignment and put increased about of stress on our joints like shoulders, knees and the lower back. Because functional exercise aims to perform exercises that are dynamic and balanced, you don’t worry about creating imbalances after the initial phase of training. Another big problem with the traditional isolation approach is it de-trains muscles form working together. This concepts of muscle coordination is important in everyday life, when you bend over to lift something, your brain sends signals to thousands of different muscles fibers to produce that movement. The key to functional exercise is about teaching all the muscles to work together rather than isolating them to work independently. In functional fitness, most of the time, you should be standing on your own two feet and supporting your own weight when you lift or execute a movement, just like real life. Are You Ready for a Functional Exercise Program? Jumping into functional exercise may startle some people used to working on machines or only running in a straight line on a treadmill for years: It's a lot harder! Not only does functional exercise work your muscles, it works your brain. It’s important to start slowly and focus on form. Receiving proper coaching and instruction is paramount to getting the most out of your workout and staying injury free. Coaching helps people understand how to use correct form (body positioning) when performing a functional exercise program. Form always comes before fatigue in a functional exercise program. I also recommend starting with little to no weight, once you can control and balance your own body weight, then you can start working with added weights. In specific instances, when someone may have a preexisting injury or continues to suffer from injury setbacks, consultation from a healthcare provider who is well educated in functional exercise may be needed. As a chiropractor and rehabilitation specialist, I always try to incorporate functional exercises into my patient’s treatment programs. Patients enjoy the functional approach, because they can see the direct improvement in their ability to perform the motions and activities that caused them the pain to begin with. They also tend to "get better" faster too. It’s empowering to help relieve a patient’s pain, but even more so to know a patient walks out my door with the strength and understanding to prevent their injury from reoccurring. |
AuthorDr. Chris Feil Archives
June 2024
Categories
All
|
 RSS Feed
RSS Feed