 Supraspinatus moving under the bony arch of the scapula Common Shoulder Pains/ Injuries: Because of the tremendous range of motion required by the shoulder to preform functional everyday tasks or recreational activities, the shoulder is highly susceptible to injury. The shoulder becomes most susceptible to repetitive injury when lifting items or when the arm is placed in an overhead position. To perform these motions without injury requires unabated shoulder range of motion and optimum shoulder stability. It does not matter how “strong” your shoulder is when posture and scapular range of motion are limited, there will be a stronger potential for shoulder injuries. Below is a list of many common injuries to the shoulder. (Note- laxity and dislocations will not be addressed in this blog post) All of these injuries occur with a similar mechanical injury mechanisms and underlying causes: Impingement: A very common injury of the shoulder is what is termed as impingement. Just like the name implies, impingement of the rotator cuff muscle (supraspinatus specifically) develops when the space between the rigid coracoacromial arch (top of the shoulder blade) and the head of the humerus (arm bone) narrows. The muscles and tendons of the rotor cuff that pass through this space begin to fray and eventually may tear because they are pinched between these hard surfaces. Why does this space narrow? Anatomically, it narrows due to bony spurs, degenerative changes, or soft-tissue thickening. Functionally, the space narrows due to dysfunctional synchronicity of the rotator cuff muscles, aberrant scapular-humeral rhythm, or faulty scapular positioning during overhead arm movements. Individuals who are predisposed to impingement have several traits that can be distinguishable by even the untrained eye. First and foremost, a susceptible person’s shoulders commonly have the appearance of being rolled forward. Everyone has seen this person before in the local gym, their workouts consists of bench pressing and more bench pressing. They look great from the front, but when you look from the side, their shoulders sickout in front of their body. Anatomically, the scapula has tipped forward and the humerus no longer sits centered in the socket of the shoulder joint. Because the head of the humerus is positioned more forward and superior in position, the individual becomes more susceptible to impingement. These postural changes lead to the described narrowing of the space for the tendons of the rotator cuff, and start the impingement process. Typically, this postural fault of the shoulder stems from tightness and shorting of the chest muscles(Pec Minor) and reciprocated weakness and lengthening of the scapular muscles that normally stabilize the scapula to the ribcage. Interestingly, almost all cadaver studies show at least some type of fraying of tendons due to impingement. Some fraying is normal over a lifetime, but many people speed this process due to poor shoulder function, leading to actual tears in the rotator cuff muscles. A full tear of a rotator cuff muscle or tendon can cause full loss of strength in specific movements and may need to be surgically fixed. 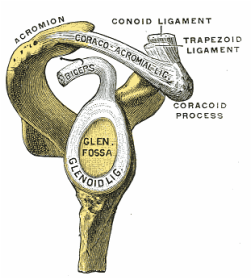 The Labrum= Glenoid Lig Bursitis In a majority of shoulder impingement cases, there is some form of bursitis involvement. Bursas are fluid filled sacs that are located throughout the body in areas of stress. They act like little pillows or shock absorbers. Most commonly they are located where a tendon travels near a bone. For example there is a bursa that is under the patellar tendon of the knee and it protects the tendon from friction with the tibia (leg bone) as it moves. There is a bursa positioned directly above the tendons of the rotator cuff in the shoulder, the “sub-acromia bursa”. When the mechanisms of impingement occur and the anatomical space narrows between the head of the humerus and scapula, not only does the tendon start to fray, but the bursa in this space is irritated. An irritated bursa will lead to an inflamed and painful bursa. When the shoulder bursa becomes inflamed, it will swell up causing even more compromise to the canal space. Many times medical doctors will inject this bursa with an anti-inflammatory to reduce the pain and swelling. But, until the mechanical stress is removed from the bursa, it will continue to become more inflamed in the future. Labral Tear - SLAP Tear The labrum gets its name from the world of architecture. In Roman architecture, a labrum was a large water-filled vessel or basin with an overhanging lip. This is actually an accurate definition of the labrum in the human shoulder. The human labrum is a layer of fibrous cartilage that surrounds the socket of bone on the scapula where the arm meets to form that shoulder joint. Because the bony socket is very shallow, the labrum adds extra depth to the socket, keeping the shoulder joint more centrated. Just like in Roman architecture, the labrum has an overhanging lip that extends around the ball head of the shoulder. The labrum in the shoulder is what we refer to as a “passive stabilizer”, meaning it relies only on its structural strength to add stability to the shoulder. The labrum has no active defense against poor posture and dysfunctional shoulder mechanics. Prolonged poor posture and faulty moments of the shoulder complex are the number 1 killers of the labrum. Weakness in the rotator cuff can also potentially lead to labral tears. The rotator cuff muscles help position the shoulder into the socket and absorb shock when functioning effectively. A dysfunctional rotator cuff will cause an increase in stress on the passive labrum. The most common injury to the labrum is a “SLAP Tear”. The technical definition is not as important as understanding the mechanism of how a tear in such a thick and strong tissue like the labrum can occur. When the shoulder is placed in a position where the humerus is not centered in the joint socket, force is not transferred effectively to the rest of the body (a break in the kinetic chain). Any force applied to a poorly positioned arm is absorbed in the joint of the shoulder, partially in the area of the labrum where the shoulder is malpositioned. As we have discussed in the mechanisms of shoulder impingement, the head of the humerus bone tends to move up and forward in the socket when impingement occurs. The same is true of a SLAP tear, SLAP is an acronym that stands for "Superior Labral tear from Anterior to Posterior” (a tear in the top front part of the shoulder labrum). Labral tears can be the cause of pain in the shoulder at night, especially if a person is a side sleeper. If there is a tear in the labrum, there will be an obvious lack of passive stability. And because the individual is asleep, their active stabilizers (the muscles) are not functioning at 100%, making the shoulder unstable when pressure is applied. In an athlete with a labral issue, the pain reported in the shoulder is a dull pain, which can cause them to loose strength when preforming overhead movements. Depending on a patient’s athletic or lifestyle goals, surgery may or may not be indicated. Simply improving the individual’s posture, mobility, and stability can sometimes do wonders for even the nastiest SLAP tear. As I always tell my patients, if you are scheduled to pitch for the Yankees tomorrow, go talk to the surgeon. Otherwise, try a few week weeks of progressive rehab first!  Bicipital Tendonitis
As I discussed in part one of the shoulder blog, the long head of the bicep and its tendon act like the fifth rotator cuff muscle. The bicep tendon travels right next to the head of the humerus, where all of the other rotator cuff muscles attach. What is unique about the bicep tendon is that it travels through a grove in the shoulder bone called the bicepital groove, very similar to the patella (kneecap) and the patellar groove. In the knee, people are often diagnosed with “patellar tracking syndrome”, meaning the kneecap shifts to the side and rubs on the bones of the knee causing pain and discomfort. A very similar mechanism happens with bicep tendon in the shoulder. As the head of the humerus bone tends to move up and forward in the socket, as is common with an individual with impingement, a greater amount of stress is applied to the bicep tendon and it will become inflamed and painful. Think of the bicep as a long rubber band that runs from the elbow to shoulder blade. When the shoulder tilts forward and the head of the humerus travels anterior (forward), this add tension to the rubber band. Individuals with bicepital tendonitis usually have increase pain when they fully extend their arm and rotate. For example, turning a door knob is where the bicepital groove comes into play. Imagine again the very tight rubber band due to poor shoulder position, now when the arm is rotated, the bony ridges of the grove run into the rubber band (inflamed tendon) that no longer has any give or play because it was pretightened. If this tendonitis happens for a long period of time, months to years, the diagnosis changes to tendonosis, which we will discuss in a future blog post. It should be noted that in specific types of SLAP tears, the ligaments that hold the bicep tendon in the grove become torn as well. This can cause a slapping sensation in the shoulder when the bicep tendon literally pops out of the groove. The Silent Tear Tears in the rotator cuff actually occur quite frequently. The scary news is that many people have tears, and don’t realize it (asymptomatic). In the general population; Sher et al. took MRIs of 96 asymptomatic subjects, finding rotator cuff tears in 34% of cases, and 54% of those older than 60. This may be why it can take very little force to cause a tremendous amount of pain in a shoulder if there is already underlining damage to the shoulder. But, on a positive note, these silent tears prove that if the shoulder mechanics (posture, mobility, and stability) are functioning properly, an individual can go throughout life without having surgery and long recovery period. In part 3 of this shoulder blog we will talk about the 3 major components of healthy shoulder mechanics in more detail, they are posture, mobility, and stability.
0 Comments
 Every good story has a villain, our Blog story’s villain is this man. Do you know who he is? He is John Smeaton, who lived in 18th century in England. He was the first self-proclaimed civil engineer, and often regarded as the "father of civil engineering". He was important in the development of modern cement, because he identified the compositional requirements needed to obtain "hydraulicity" in lime; his work which led ultimately to the invention of Portland cement. Portland cement led to the re-emergence of concrete. Cement is a good thing right? Not for your feet. By the 18th century modern man knew that the world was round, but that didn’t stop John Smeaton, he made the world flat again! Think about a day in the life for your feet in this modern flat and hard world. Your first step out of bed is on to a flat surface (assuming you clean your room), when you leave your flat surfaced house in the morning you walk outside on to cement and asphalt to your car. Your place of employment is most likely built on a cement slab. It may seem counterintuitive, but standing on a hard flat surface all day maybe the worst thing you can do to your feet. Your feet are meant to be mobile adaptors to the ground. Think of primitive human’s fist walking the savanna, adapting every step. Human’s feet developed this way for thousands of years and became adaptive and incredibly efficient.  Ancient man’s feet where stronger, and wider then modern man’s feet when we compare fossilized artifacts. We can also assume that ancient man’s feet were more mobile than ours as well. Constantly walking on uneven surfaces would naturally mobilize all of the 31 different joints in the human foot. All of this foot movement was also good for the nervous system. The human foot is the second most sensitive area in your body. There are thousands of nerve endings in the foot that detect the slightest change in the ground surface and send that information to the brain. (The next time you need to act in self-defense, it is actually much more debilitating to stomp on someone’s foot). The ground we walk on today does not challenge the muscles, ligaments, joints, or nerves of the foot. The old saying goes “use it or lose it”; this definitely applies to our feet. The joints stiffen, the muscles shorten from inactivity and become weak, and our brain doesn’t get the sensory information it needs to coordinate our foot movements. What is even worse is that over the last 30-40 years, we have started housing our feet in little day spas called athletic shoes. The EVO foam within shoes dampens the sensory input into our feet even more. The trend has also been to add more motion control to shoes, again limiting the foot’s natural ability to move. This ongoing cycle of foot weaknesses and under-stimulation may have caused the recent wave of minimalist shoes to hit the market the last few years.  Minimalist Shoe Revolution Now the running and fitness word is in the start of the minimalist shoe revolution. A Blogger defines the three criteria for the perfect minimalist shoe: 1) Allows for maximum proprioception for the intended purpose. The purpose defines the trade-offs necessary for thermal and puncture protection. 2) Allows for appropriate shifts in the body’s center of gravity in terms of sole thickness and heel to toe differential. 3) Allows for complete natural movement of the foot in terms of room and flexibility for bone structure and elasticity as well as proper heat dissipation. Philosophically, minimalist shoes are a great idea if you lived your life on an Amish farm inthe middle of Pennsylvania your whole life. But, most of us have lived our whole lives in athletic shoes walking and exercising in a hard flat world of cement and concrete. We have been literally trained to live in shoes, and our foot morphology has changed. The good news is, your feet can change back, but it takes time. Going cold turkey never works, a runner needs a plan before starting to wearing minimalist shoes. Potential Injuries If someone makes too dramatic of a change to minimalist shoe or barefoot, several injuries can occur. The most common complaints of runner who switches to minimalist shoes are plantar fasciitis and Achilles tendon injuries. Both of the mechanisms related to these injuries are due to overloading of tissues that may have been shortened due to years of running with an elevated heal. Typically, minimalist footwear have close to a zero drop, meaning when standing flat on the ground there is the same height difference from the ball of your foot to the ground as there is from the heel of your foot. The extra few millimeters that the heel must travel to hit the ground may not seemlike much in a zero drop shoe. But, repetitively making the tissues of the plantar fascia and Achilles tendon stretch thousands of times during a simple 3-5 mile jog can easily lead to an injury. Not as common, but very serious injury associated with minimalist running are tribal stress fractures. Military research discovered that soldiers with high supinated arches are more likely to have a stress fractures marching while in basic training. Like the military study, switching to a midfoot landing is much like mechanics of marching; therefor the risk of stress fractures might be the same in someone with a ridged foot. It is my belief that when a runner switches to a minimalist shoe, often their running technique changes. Like learning any new skill, you will have flaws in your gait pattern initially. The problem with minimalist shoes is that if you are running on hard surfaces, there is no room for error with a minimalist shoe because of its lack of built in shock absorption and fractures may happen. Another potential problem with running in minimalist shoe is discussed in Dr. Thomas Michaud’s book Human Locomotion. Permanent injury may occur to a runners heel pad by running on cement/asphalt barefoot or with a minimalist shoe, especially when still using a heel strike. Unfortunately, if you damage the fat pad in your heel, it may never heal and can lead to chronic pain. 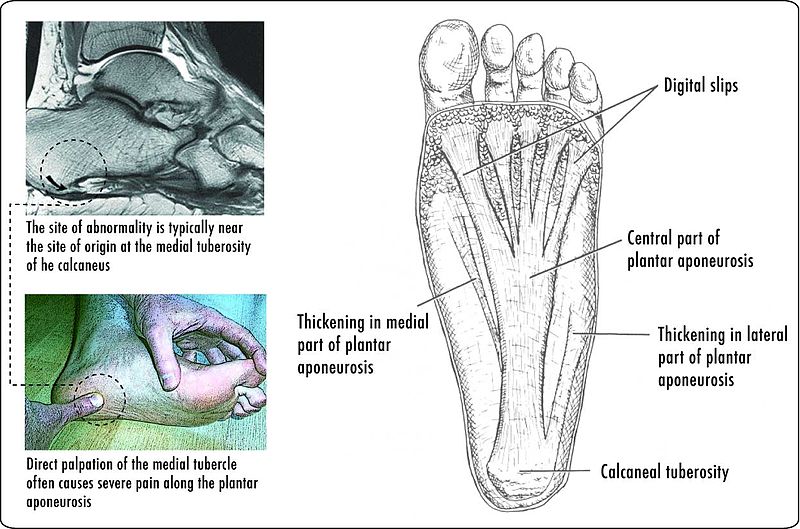 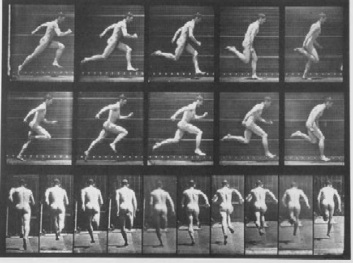 Minimalist Shoe Transition Recommendations
My recommendation for switching to minimalist shoe is building in a large transition zone to prevent injury and give your body and feet a time to adapt. Before someone goes out a buys a minimalist shoe, I would consult an expert in the field of gait and sports medicine, like myself (shameless self-promotion warning). A proper biomechanical evaluation should be performed to see if switching shoes is appropriate for you. Individuals may need to preform exercises and stretches prior to even attempting the switch to minimalist shoes. To begin the transition to minimalist shoes, an individual should start by wearing the minimalist shoes around their house for a week, prior to running. The first few weeks of running in the minimalist shoes should be performed by alternating running days in traditional shoes and the new minimalist shoes. Distances should build very gradually with minimalist shoes. It may take several weeks to run three miles in a minimalist shoe even if you are used to ten mile runs in traditional shoes. Training on softer surfaces like dirt or grass can also degrees the new stresses associated with minimalist shoe running. Another smart idea when switching to minimalist shoes is not jumping in to a shoe like an aggressive Vibrum Five Finger first. They have started to sell hybrid models that give your body more time to adapt to the gait changes and mechanical changes associated with minimalist shoed running. If you continue to plan to do the majority of your running on hard surfaces, invest in a hybrid shoe( like a Saucony Kinvara) for your long run days and then wear a true minimalist shoe for the light training days. Minimalist Shoe Gait Changes There are a few typical changes in gait mechanics observed in gait mechanics when a person starts to run and train in minimalist shoes. First and the most significant change noticed is in the contact zone of the foot on initial foot strike. Whereas traditional running shoes with a high heel and a positive drop, cause runners to inherently contact the ground with their heel first. (This heal contact will be addressed in future blog posts.) Wearing a minimalist usually leads to a midfoot or forefoot strike. Minimalist shoed runners also have a higher cadence in running. An average recreational runner may have a cadence of 120 steps a minute; by switching to a minimalist shoe a runner’s cadence may increase to 150-160 steps a minute. This increase in cadence is caused by three factors. First, minimalist runners shorten their stride length, or more importantly they don’t over stride. Second, minimalist shoe runners decrease their vertical elevation while running (decreasing ground reaction forces). Lastly, minimalist runner’s shoes are much lighter than even the lightest traditional running shoe. The proven benefits to running in a minimalist shoe are: smoother ground impacts, maximum shoe and foot flexibility, increased traction, increased sensory input in your foot (proprioception), increased toe function, and finally it gives the runner more of a chance to self-analyze and “feel” their running gait mechanics. Because the protective shock absorption is gone from the traditional running shoe, the minimalist shoe runner really feels every step (proprioception). Subconsciously, the runner will intuitively find ways to reduce the stress of running by changing their gait mechanics. I think it is important to note that shoes are just tools. Man’s ability to use tools has set our species apart for the rest of the animal kingdom. But, our use of tools is not without mistakes and failures along the way. Ideally, everyone should be able to put on a minimalist shoe and run a 5k and feel great. Unfortunately, that’s not possible because our bodies have adapted to our surroundings. We are used to wearing traditional running shoes and our running and daily walking surfaces are hard and flat. This is not the minimalist shoes fault, but it is an undeniable truth we must accept. I hope this blog helps with some of the questions runners in Ames, Iowa may have about minimalist shoes. (Images are CC from Wikipedia: By Brett L. (originally posted to Flickr as Mai's amazing socks) [CC-BY-SA-2.0 (http://creativecommons.org/licenses/by-sa/2.0)], via Wikimedia Commons and Homo heidelbergensis - Author= Jose Luis Martinez) Understanding the Shoulder Complex and its Relationship with the Rest of the Body: The human shoulder is one of the most dynamic joints in the body. It is essential to have healthy shoulder mechanics to perform well in athletics, but also to preform activities of daily living. Shoulder health is often determined by the relationship between the shoulder and the rest of the body. Unfortunately, there are several factors that compromise that relationship and lead to shoulder injuries. I believe the three factors that lead to shoulder dysfunction are: posture, mobility, and stability. Stats: Statistically there is a high prevalence of shoulder injuries in America. In 2006, approximately 7.5 million people went to the doctor's office for a shoulder problem; more than 4.1 million of these visits were for rotator cuff problems. (orthoinfo.com) Shoulder injuries are the second most common injury to cause missed work time, lower back injuries are credited as the number one reason people miss time at work. However, shoulder injuries take the most time to recover and return to work, compared to other injuries. On average it takes 30 days to return to work after a shoulder injury compared to 13 days after a back injury. (TDI, TWC) Anatomy: The primary joint people think of when they talk about the shoulder is the “glonohumaral joint” this is the ball and socket joint that attaches the humerus (arm bone) to the scapula (shoulder blade). The best analogy of this joint is of a golf ball on a tee. The bony joint surface that connects the humerus to the scapula is not much bigger than the size of the head of a golf tee. The stability of the joint is mainly gained through soft tissues, meaning the ligaments, tendons, and muscles that surround the shoulder. The soft tissues try to keep the head of the humerus centered on the scapula; this concept is called centration and is fundamental to preventing injuries.  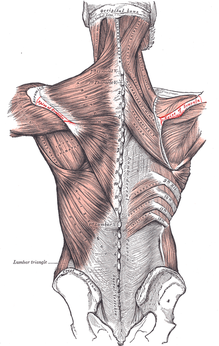 The first layer on top of the bone is a covering of ligaments including the labrum and the shoulder joint capsule. On top of the shoulder capsule are the muscles and tendons of the rotator cuff. Technically the rotator cuff consists of 4 muscles: supraspinatus, infraspinatus, teres minor, and the often forgotten subscapularus. The cuff muscles attach on the head of the humerus and originate from the scapula. I often include the long head of the biceps in the group of the rotator cuff because of its proximity and function in shoulder stabilization. The muscles of the cuff must perform several tasks to aid in shoulder function. Each of the muscles moves the shoulder in a specific direction. For example, supraspinatus raises the arm overhead after the shoulder has reached 90 degrees. When a person injures their supraspinatus, they are not able to lift their arm over their shoulder. Possibly the most important task of the rotator cuff is to stabilize the head of the humerus. There are constant small contractions from all of the cuff muscles to keep the head of the humorous centrated. The final layer of protection comes from the muscles that stabilize the scapula. There are a total of 18 muscles that attach to the scapula. Most of the muscles that attach to the scapula originate from the spine and ribcage. This group of muscles help move and stabilize the scapula. If the scapula does not move effectively or there is a weakness in the muscles supporting the scapula,increased stress is placed on the shoulder and the cuff muscles. Without scapular motion, humans would not be able to raise their arms over 120 degrees. It becomes imperative that middle back, lower neck, and rib cage be mobile to allow the shoulder blade to move to reduce stress on the shoulder. Video By Young Lae, Moon M.D. Chair of 3D Based Medical Application Working group.
Chairman and Professor of Orthopaedics, Chosun University Hospital, Korea. [CC-BY-3.0 (http://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons By Dr. Chris Feil, Team Chiropractic and Rehabilitation of Ames It has always puzzled me why when we sit at work all day, why people want to go to the gym and sit more while they work out? The concept of functional exercise has turned that idea of static isolated exercise upside down! Functional Exercises principles focus on building a body capable of doing real-life activities in real-life positions, not just lifting a certain amount of weight in a static posture created by a gym machine. Functional exercises tend to be multi-joint and multi-muscle exercises, or what we call compound movements. Instead of only moving the elbows, for example, a functional exercise might involve the elbows, shoulders, spine, hips, knees and ankles. Not only is functional exercise fun, because you are up moving around, you also get the benefit of exercising at higher intensities because you are using all the muscles in your body during the whole workout. The more muscles you use, the more calories you burn! Also, by performing exercises like kettelbells and kickboxing that use several muscles groups, you start to train the neglected areas of your body, without even thinking about it. Neglected areas, like your middle back, hips, abdominals, and even your feet. When these areas are strong, they help prevent injuries and make exercise and your everyday activities easer. Where did the Traditional American Gyms Go Wrong? Today traditional American gym workouts often focus on isolating and challenging one specific muscle. Usually, one movement of a joint is preformed in a controlled range of motion, while the rest of your body’s muscles remain static and dormant. This mindset comes from the body building culture. When Arnold Schwarzenegger needed to tone each individual muscle, he and his friends devised sets of specific exercise to make their muscles "bulge" when he flexed on stage or in the movies. There are several problems with that approach; traditionally bodybuilding overdevelops certain muscles, like the chest muscles, biceps and quads. When these muscle groups become too strong and out of balance with the rest of our bodies, they pull our posture out of alignment and put increased about of stress on our joints like shoulders, knees and the lower back. Because functional exercise aims to perform exercises that are dynamic and balanced, you don’t worry about creating imbalances after the initial phase of training. Another big problem with the traditional isolation approach is it de-trains muscles form working together. This concepts of muscle coordination is important in everyday life, when you bend over to lift something, your brain sends signals to thousands of different muscles fibers to produce that movement. The key to functional exercise is about teaching all the muscles to work together rather than isolating them to work independently. In functional fitness, most of the time, you should be standing on your own two feet and supporting your own weight when you lift or execute a movement, just like real life. Are You Ready for a Functional Exercise Program? Jumping into functional exercise may startle some people used to working on machines or only running in a straight line on a treadmill for years: It's a lot harder! Not only does functional exercise work your muscles, it works your brain. It’s important to start slowly and focus on form. Receiving proper coaching and instruction is paramount to getting the most out of your workout and staying injury free. Coaching helps people understand how to use correct form (body positioning) when performing a functional exercise program. Form always comes before fatigue in a functional exercise program. I also recommend starting with little to no weight, once you can control and balance your own body weight, then you can start working with added weights. In specific instances, when someone may have a preexisting injury or continues to suffer from injury setbacks, consultation from a healthcare provider who is well educated in functional exercise may be needed. As a chiropractor and rehabilitation specialist, I always try to incorporate functional exercises into my patient’s treatment programs. Patients enjoy the functional approach, because they can see the direct improvement in their ability to perform the motions and activities that caused them the pain to begin with. They also tend to "get better" faster too. It’s empowering to help relieve a patient’s pain, but even more so to know a patient walks out my door with the strength and understanding to prevent their injury from reoccurring. |
AuthorDr. Chris Feil Archives
June 2024
Categories
All
|
 RSS Feed
RSS Feed