|
If the internet has done one thing for the world, it has made average people into “experts” on almost any topic with just a few clicks. My personal area of internet pseudo expertise is in the field of auto mechanics (just ask my wife how many times I’ve tried to save money fixing the car myself). It seems so easy on Youtube, and message boards always have creditable information, right? The same can be said for fitness and sport injuries information on the web. I believe the majority of content on the web is generally reliable (you are most likely reading this online), the problem starts when fundamentals are glossed over or basic concepts are assumed. In the world of functional exercise a great deal of attention is placed on athlete’s injuries, but not enough time and emphasis is spent on correct posture to prevent injuries. As fitness coaches and organizations push to continually challenge and vary workouts, one of the undervalued fundamentals of shoulder and spinal health, is the posture of the thoracic cage. I believe if coaches and athletes spent more time focusing on the posture and movement of the thoracic cage during exercise, several shoulder and spinal injuries could be prevented. Believe it or not, by simply observing the positioning (posture) of the thoracic cage prior to an individual preforming an exercise, you can estimate how successful they will be at performing the exercise.  My novice ability to fix a car is the perfect analogy as to why the position of the thoracic cage is so important during exercise. A few years back I needed new brake pads for my car, so I pulled up a trusty YouTube video, ordered my parts online, and took on the automotive challenge in the driveway of my new house. As I jacked up the car, I failed to notice that the driveway at our new house had a slight slope compared to our old driveway. Just as I removed the second front tire, the car began to slowly lean backwards. I jumped away as the car slipped off the car jack and crashed to the ground. In this analogy, the sloped driveway represents the thoracic cage, the jack represents the scapula (shoulder blade), and the car is the shoulder. In the rehab world, a great deal of emphasis is placed on “scapular stability” to help injured shoulders. I am here to tell you that scapular stability is functionally impossible to obtain if the thoracic cage is out of position. The bigger the slope in the driveway, the more unstable the car jack is! The thoracic cage consists of the spinal bones of the mid back (thoracic spine), the attaching ribs, and all of the muscles that attach to the bones and cartilage. The accepted term for faulty positioning of the thoracic cage is a “rib flare”. 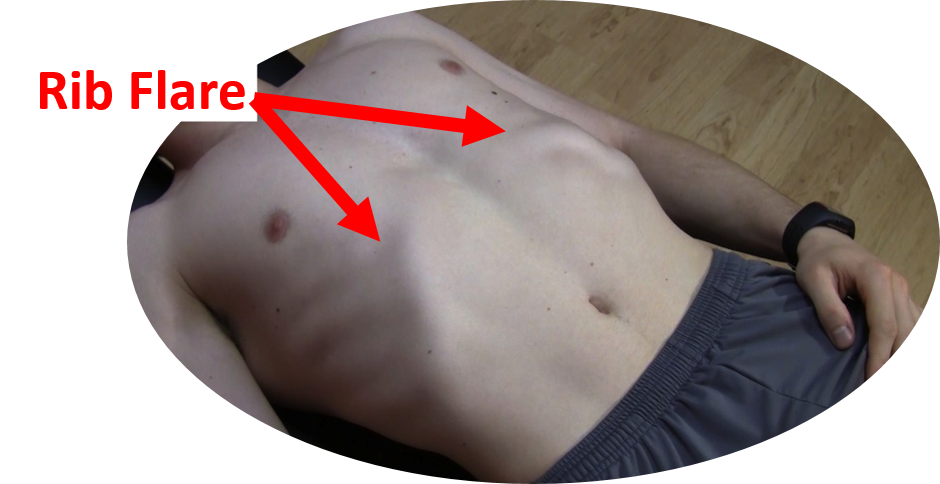 Picture taking a deep breath into your lungs and holding it, the resulting rib position would be an example of a rib flare. The entire ribcage is elevated and the base of the front of the rib cage is protrudes forward and out. Functionally this causes a lot of compromise in the body:
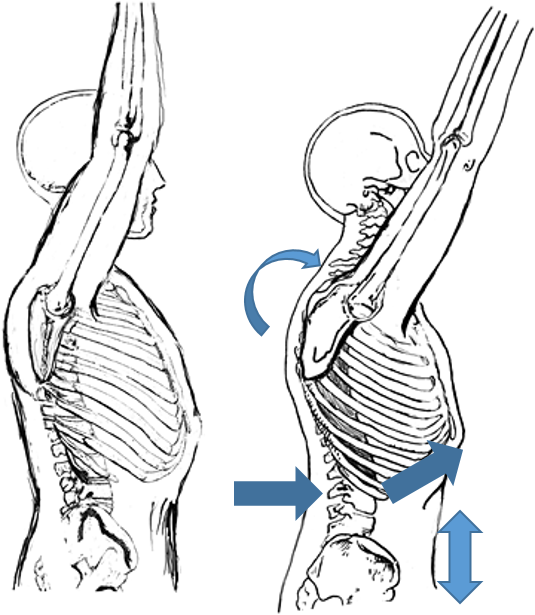 Why does a rib flare commonly occur in functional exercises like pull-ups, squats, push ups and overhead pressing? I think the number one reason people continue to exercise with a rib flare is that it provides “passive” stability when preforming explosive movements. “Active” stability is achieved by correct activation of stabilizing muscle groups in the region. For example, the abdominals and the muscles of the mid back. If the stabilizing muscle groups are inactive or weak, athletes will start to use the end range positions of their joints to provide a base of support for their body as they exercise. Meaning: the lower back joints lock into hyperextension and a rib flare causes the thoracic cage to become rigid and compressed, all to make up for a lack of active muscular stability. There are a few problems with this postural fault:
When I went back and re-watched the automotive Youtube videos after dropping my car, of course I saw there were blocks behind the tires when they jacked up their car. A slight detail that I originally overlooked. Now, anytime that I jack up the car, I place blocks under the tires to prevent the car from rolling down the driveway again. Going back to the shoulder analogy, the “tire blocks” represent our rotator cuff muscles. The number one job of the cuff muscles is to keep the shoulder stable in its socket. Athletes always ask me why their cuff muscles are tight and sore. I tell them it’s because of their posture; they usually give me a funny look. After a few visits they start to understand positioning the thoracic cage correctly during activity, enables the scapulae to stabilize in the thoracic wall, greatly reducing the stress in the lumbar spine and rotator cuffs. Correcting a rib flare may be as simple as tightening the core muscles to pull the rib cage back down prior to and during an exercise. But, in an athlete that has had a rib flare for several years, it may take longer to correct the problem. First they have to regain the mobility of the thoracic spine and rib cage. The best way to combat a long-term postural problem is a ton of foam rolling (don’t forget to roll out the ribs) and dynamic mobility exercises. The mobility exercises must be followed up with a retraining program targeting core/glute/ and scapular muscle activation and strength. Video analysis can be used to help the athlete visualize correct posture during exercise too. In summary- Strengthen your core and do more mobility work on your thoracic cage. Do not constantly hyperextend your lower back and flare your ribs when exercising Be sure to pay attention to details, and most importantly, never let me fix your car! By Dr. Chris Feil
9 Comments

Believe it or not, when you were 10 months old, you probably had better push-up form/technique then you do now! How can that be? It’s actually quite simple, a healthy infant trains their stabilizing muscles all day long. They do this by the simple act of crawling. When you think about it, spending all day on your hands and knees does wonders for developing the muscles that run from your back and ribs to your shoulder blades (scapula), these muscles are what we in the rehab community call scapular stabilizers. Specifically, the scapular stabilizing muscles are: lower trapezius, serratus anterior, and rhomboids. Unfortunately these muscles are often underdeveloped and neglected.
As we get older, we tend to stop using the scapular stabilizing group of muscles in our modern lives. We spend hours sitting or standing with sometimes not so great posture. Even people that “go to the gym”, may not have an adequate ability to control their scapula because many of the exercises they preform are pushing exercises (there is a difference between a bench press and a push-up functionally). It is not coincidence that many of my patients that have shoulder pain and or neck pain/mid back, have tight chest muscles (Pec and Pec minor) and tight muscle that run from the neck to the shoulder (upper trapezius and levator scapula). Typically these muscles tighten because the scapular stabilizing muscles are under developed and under-utilized, leading to a rounding of the shoulders and an observable “winging” or elevation of the shoulder blades. Back to the baby push-ups to crawl effectively an infant must be able to keep their shoulder blades “glued” to their rib cage. This allows them to shift their body weight from one arm to the other as they pivot and crawl forward. Without this ability to stabilize their scapula, they would not be able to move from one arm to another while holding up their body. This concept of scapula hugging the rib cage is the big difference between a proper push-up and an exercise like a bench press. Bench pressing is grasping a weight and moving your hands up and down, actually the opposite motion of a push-up functionally. Preforming a proper push-up is really about using your shoulder blades to lift your torso up and down, much like the infant uses the shoulder blade to control the body while crawling. The concept may seem simple, but most people focus on their arms and hands too much when preforming push-ups and actually put their shoulders in a compromised position leading to increased strain on the shoulder and eventually impairment. Instead, focus on the tips below to help you revert back to your perfect baby style push-ups: · Start on the ground perfectly flat, lift the hands up of the ground and squeeze the shoulders blades down and back. (Keep the shoulder blades glued to the rib cages during the whole push-up movement) · Place the hands on the ground using a narrow hand position · Keep the hands below the plane of your shoulders · Direct the crease of your elbows forward (toward the direction of your head) as you push up · Shift the weight in your hands off the index finger and thumb to a more balanced palm pressure · Keep your pelvis and lower back in a neutral position · Keep your chin tucked in and your head retracted back.  Supraspinatus moving under the bony arch of the scapula Common Shoulder Pains/ Injuries: Because of the tremendous range of motion required by the shoulder to preform functional everyday tasks or recreational activities, the shoulder is highly susceptible to injury. The shoulder becomes most susceptible to repetitive injury when lifting items or when the arm is placed in an overhead position. To perform these motions without injury requires unabated shoulder range of motion and optimum shoulder stability. It does not matter how “strong” your shoulder is when posture and scapular range of motion are limited, there will be a stronger potential for shoulder injuries. Below is a list of many common injuries to the shoulder. (Note- laxity and dislocations will not be addressed in this blog post) All of these injuries occur with a similar mechanical injury mechanisms and underlying causes: Impingement: A very common injury of the shoulder is what is termed as impingement. Just like the name implies, impingement of the rotator cuff muscle (supraspinatus specifically) develops when the space between the rigid coracoacromial arch (top of the shoulder blade) and the head of the humerus (arm bone) narrows. The muscles and tendons of the rotor cuff that pass through this space begin to fray and eventually may tear because they are pinched between these hard surfaces. Why does this space narrow? Anatomically, it narrows due to bony spurs, degenerative changes, or soft-tissue thickening. Functionally, the space narrows due to dysfunctional synchronicity of the rotator cuff muscles, aberrant scapular-humeral rhythm, or faulty scapular positioning during overhead arm movements. Individuals who are predisposed to impingement have several traits that can be distinguishable by even the untrained eye. First and foremost, a susceptible person’s shoulders commonly have the appearance of being rolled forward. Everyone has seen this person before in the local gym, their workouts consists of bench pressing and more bench pressing. They look great from the front, but when you look from the side, their shoulders sickout in front of their body. Anatomically, the scapula has tipped forward and the humerus no longer sits centered in the socket of the shoulder joint. Because the head of the humerus is positioned more forward and superior in position, the individual becomes more susceptible to impingement. These postural changes lead to the described narrowing of the space for the tendons of the rotator cuff, and start the impingement process. Typically, this postural fault of the shoulder stems from tightness and shorting of the chest muscles(Pec Minor) and reciprocated weakness and lengthening of the scapular muscles that normally stabilize the scapula to the ribcage. Interestingly, almost all cadaver studies show at least some type of fraying of tendons due to impingement. Some fraying is normal over a lifetime, but many people speed this process due to poor shoulder function, leading to actual tears in the rotator cuff muscles. A full tear of a rotator cuff muscle or tendon can cause full loss of strength in specific movements and may need to be surgically fixed. 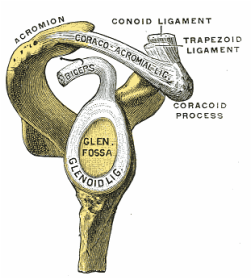 The Labrum= Glenoid Lig Bursitis In a majority of shoulder impingement cases, there is some form of bursitis involvement. Bursas are fluid filled sacs that are located throughout the body in areas of stress. They act like little pillows or shock absorbers. Most commonly they are located where a tendon travels near a bone. For example there is a bursa that is under the patellar tendon of the knee and it protects the tendon from friction with the tibia (leg bone) as it moves. There is a bursa positioned directly above the tendons of the rotator cuff in the shoulder, the “sub-acromia bursa”. When the mechanisms of impingement occur and the anatomical space narrows between the head of the humerus and scapula, not only does the tendon start to fray, but the bursa in this space is irritated. An irritated bursa will lead to an inflamed and painful bursa. When the shoulder bursa becomes inflamed, it will swell up causing even more compromise to the canal space. Many times medical doctors will inject this bursa with an anti-inflammatory to reduce the pain and swelling. But, until the mechanical stress is removed from the bursa, it will continue to become more inflamed in the future. Labral Tear - SLAP Tear The labrum gets its name from the world of architecture. In Roman architecture, a labrum was a large water-filled vessel or basin with an overhanging lip. This is actually an accurate definition of the labrum in the human shoulder. The human labrum is a layer of fibrous cartilage that surrounds the socket of bone on the scapula where the arm meets to form that shoulder joint. Because the bony socket is very shallow, the labrum adds extra depth to the socket, keeping the shoulder joint more centrated. Just like in Roman architecture, the labrum has an overhanging lip that extends around the ball head of the shoulder. The labrum in the shoulder is what we refer to as a “passive stabilizer”, meaning it relies only on its structural strength to add stability to the shoulder. The labrum has no active defense against poor posture and dysfunctional shoulder mechanics. Prolonged poor posture and faulty moments of the shoulder complex are the number 1 killers of the labrum. Weakness in the rotator cuff can also potentially lead to labral tears. The rotator cuff muscles help position the shoulder into the socket and absorb shock when functioning effectively. A dysfunctional rotator cuff will cause an increase in stress on the passive labrum. The most common injury to the labrum is a “SLAP Tear”. The technical definition is not as important as understanding the mechanism of how a tear in such a thick and strong tissue like the labrum can occur. When the shoulder is placed in a position where the humerus is not centered in the joint socket, force is not transferred effectively to the rest of the body (a break in the kinetic chain). Any force applied to a poorly positioned arm is absorbed in the joint of the shoulder, partially in the area of the labrum where the shoulder is malpositioned. As we have discussed in the mechanisms of shoulder impingement, the head of the humerus bone tends to move up and forward in the socket when impingement occurs. The same is true of a SLAP tear, SLAP is an acronym that stands for "Superior Labral tear from Anterior to Posterior” (a tear in the top front part of the shoulder labrum). Labral tears can be the cause of pain in the shoulder at night, especially if a person is a side sleeper. If there is a tear in the labrum, there will be an obvious lack of passive stability. And because the individual is asleep, their active stabilizers (the muscles) are not functioning at 100%, making the shoulder unstable when pressure is applied. In an athlete with a labral issue, the pain reported in the shoulder is a dull pain, which can cause them to loose strength when preforming overhead movements. Depending on a patient’s athletic or lifestyle goals, surgery may or may not be indicated. Simply improving the individual’s posture, mobility, and stability can sometimes do wonders for even the nastiest SLAP tear. As I always tell my patients, if you are scheduled to pitch for the Yankees tomorrow, go talk to the surgeon. Otherwise, try a few week weeks of progressive rehab first!  Bicipital Tendonitis
As I discussed in part one of the shoulder blog, the long head of the bicep and its tendon act like the fifth rotator cuff muscle. The bicep tendon travels right next to the head of the humerus, where all of the other rotator cuff muscles attach. What is unique about the bicep tendon is that it travels through a grove in the shoulder bone called the bicepital groove, very similar to the patella (kneecap) and the patellar groove. In the knee, people are often diagnosed with “patellar tracking syndrome”, meaning the kneecap shifts to the side and rubs on the bones of the knee causing pain and discomfort. A very similar mechanism happens with bicep tendon in the shoulder. As the head of the humerus bone tends to move up and forward in the socket, as is common with an individual with impingement, a greater amount of stress is applied to the bicep tendon and it will become inflamed and painful. Think of the bicep as a long rubber band that runs from the elbow to shoulder blade. When the shoulder tilts forward and the head of the humerus travels anterior (forward), this add tension to the rubber band. Individuals with bicepital tendonitis usually have increase pain when they fully extend their arm and rotate. For example, turning a door knob is where the bicepital groove comes into play. Imagine again the very tight rubber band due to poor shoulder position, now when the arm is rotated, the bony ridges of the grove run into the rubber band (inflamed tendon) that no longer has any give or play because it was pretightened. If this tendonitis happens for a long period of time, months to years, the diagnosis changes to tendonosis, which we will discuss in a future blog post. It should be noted that in specific types of SLAP tears, the ligaments that hold the bicep tendon in the grove become torn as well. This can cause a slapping sensation in the shoulder when the bicep tendon literally pops out of the groove. The Silent Tear Tears in the rotator cuff actually occur quite frequently. The scary news is that many people have tears, and don’t realize it (asymptomatic). In the general population; Sher et al. took MRIs of 96 asymptomatic subjects, finding rotator cuff tears in 34% of cases, and 54% of those older than 60. This may be why it can take very little force to cause a tremendous amount of pain in a shoulder if there is already underlining damage to the shoulder. But, on a positive note, these silent tears prove that if the shoulder mechanics (posture, mobility, and stability) are functioning properly, an individual can go throughout life without having surgery and long recovery period. In part 3 of this shoulder blog we will talk about the 3 major components of healthy shoulder mechanics in more detail, they are posture, mobility, and stability. Understanding the Shoulder Complex and its Relationship with the Rest of the Body: The human shoulder is one of the most dynamic joints in the body. It is essential to have healthy shoulder mechanics to perform well in athletics, but also to preform activities of daily living. Shoulder health is often determined by the relationship between the shoulder and the rest of the body. Unfortunately, there are several factors that compromise that relationship and lead to shoulder injuries. I believe the three factors that lead to shoulder dysfunction are: posture, mobility, and stability. Stats: Statistically there is a high prevalence of shoulder injuries in America. In 2006, approximately 7.5 million people went to the doctor's office for a shoulder problem; more than 4.1 million of these visits were for rotator cuff problems. (orthoinfo.com) Shoulder injuries are the second most common injury to cause missed work time, lower back injuries are credited as the number one reason people miss time at work. However, shoulder injuries take the most time to recover and return to work, compared to other injuries. On average it takes 30 days to return to work after a shoulder injury compared to 13 days after a back injury. (TDI, TWC) Anatomy: The primary joint people think of when they talk about the shoulder is the “glonohumaral joint” this is the ball and socket joint that attaches the humerus (arm bone) to the scapula (shoulder blade). The best analogy of this joint is of a golf ball on a tee. The bony joint surface that connects the humerus to the scapula is not much bigger than the size of the head of a golf tee. The stability of the joint is mainly gained through soft tissues, meaning the ligaments, tendons, and muscles that surround the shoulder. The soft tissues try to keep the head of the humerus centered on the scapula; this concept is called centration and is fundamental to preventing injuries.  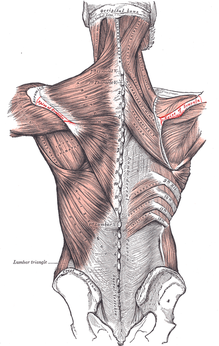 The first layer on top of the bone is a covering of ligaments including the labrum and the shoulder joint capsule. On top of the shoulder capsule are the muscles and tendons of the rotator cuff. Technically the rotator cuff consists of 4 muscles: supraspinatus, infraspinatus, teres minor, and the often forgotten subscapularus. The cuff muscles attach on the head of the humerus and originate from the scapula. I often include the long head of the biceps in the group of the rotator cuff because of its proximity and function in shoulder stabilization. The muscles of the cuff must perform several tasks to aid in shoulder function. Each of the muscles moves the shoulder in a specific direction. For example, supraspinatus raises the arm overhead after the shoulder has reached 90 degrees. When a person injures their supraspinatus, they are not able to lift their arm over their shoulder. Possibly the most important task of the rotator cuff is to stabilize the head of the humerus. There are constant small contractions from all of the cuff muscles to keep the head of the humorous centrated. The final layer of protection comes from the muscles that stabilize the scapula. There are a total of 18 muscles that attach to the scapula. Most of the muscles that attach to the scapula originate from the spine and ribcage. This group of muscles help move and stabilize the scapula. If the scapula does not move effectively or there is a weakness in the muscles supporting the scapula,increased stress is placed on the shoulder and the cuff muscles. Without scapular motion, humans would not be able to raise their arms over 120 degrees. It becomes imperative that middle back, lower neck, and rib cage be mobile to allow the shoulder blade to move to reduce stress on the shoulder. Video By Young Lae, Moon M.D. Chair of 3D Based Medical Application Working group.
Chairman and Professor of Orthopaedics, Chosun University Hospital, Korea. [CC-BY-3.0 (http://creativecommons.org/licenses/by/3.0)], via Wikimedia Commons |
AuthorDr. Chris Feil Archives
June 2024
Categories
All
|
 RSS Feed
RSS Feed